

Mortality in polymyalgia rheumatica: a 38-year prospective population-based cohort study from Southern Norway
- PMID: 40691638
- PMCID: PMC12278481
- DOI: 10.1186/s13075-025-03613-9
Mortality in polymyalgia rheumatica: a 38-year prospective population-based cohort study from Southern Norway
Abstract
Background: Robust long-term mortality data on patients with polymyalgia rheumatica (PMR) are lacking. The aim of this study was to determine all-cause mortality in isolated PMR using a large, population-based, inception cohort followed prospectively over a 38-year period.
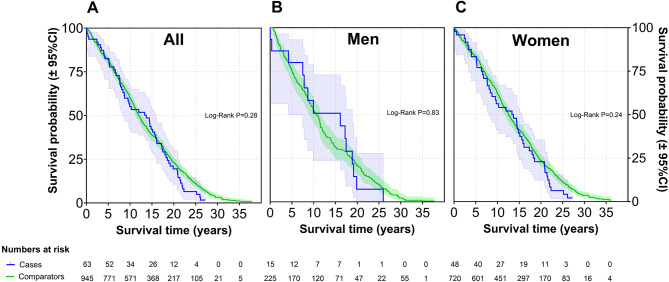
Methods: Between 1987 and 1997, 337 incident cases of PMR and biopsy-proven GCA were included in a prospective, population-based inception cohort in Aust-Agder County, Norway. Diagnosis was ascertained clinically by a rheumatologist, with PMR cases meeting Bird`s criteria. Patients were followed until death or end of study on December 31st, 2024. Each case was matched by gender, age at inclusion, and residency with 15 population comparators drawn from the population registry in Norway. We assessed mortality and survival by standard mortality ratios (SMR) and the Kaplan-Meier method.
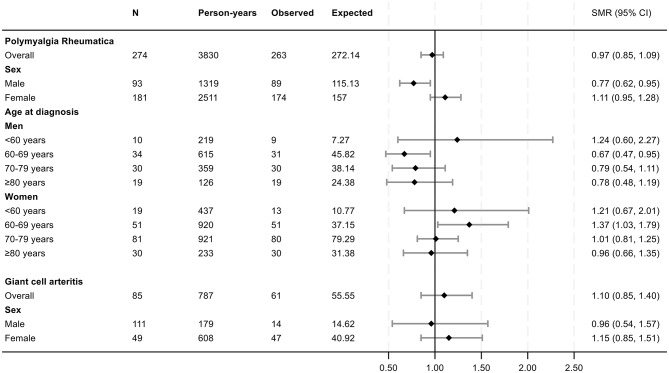
Results: A total of 274 patients with isolated PMR (66.1% female, mean age at diagnosis 71.9 years) and 63 patients with GCA (76.2% female, mean age at diagnosis 71.6 years) were included. By the end of the study, 96.4% of all patients were deceased. Mean follow-up time for all patients was 13.7 years, with a maximum of 35.3 years. For cases with isolated PMR, the overall SMR was 0.97 (95% confidence interval [CI] 0.85, 1.09), for men 0.77 (95% CI 0.62, 0.95), and for women 1.11 (95% CI 0.95, 1.28). For GCA, the overall SMR was 1.10 (95% CI 0.85, 1.40), with no gender difference.
Conclusions: In this comprehensive long-term follow-up study with nearly complete data on mortality, isolated PMR was not associated with increased mortality, reinforcing the view that it does not confer a higher mortality risk.
Keywords: Epidemiology; Giant cell arteritis; Mortality; Polymyalgia rheumatica; Survival.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study complies with the Declaration of Helsinki and was approved by the regional ethics committee with exemption from informed consent for identifications of patients and linkage to the NPR (Case number 45964, November 14, 2019). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Polymyalgia rheumatica and giant cell arteritis induced by immune checkpoint inhibitors: A systematic literature review highlighting differences from the idiopathic forms.Autoimmun Rev. 2024 Jul-Aug;23(7-8):103589. doi: 10.1016/j.autrev.2024.103589. Epub 2024 Aug 6. Autoimmun Rev. 2024. PMID: 39117006
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
-
Effect of Tocilizumab on Disease Activity in Patients With Active Polymyalgia Rheumatica Receiving Glucocorticoid Therapy: A Randomized Clinical Trial.JAMA. 2022 Sep 20;328(11):1053-1062. doi: 10.1001/jama.2022.15459. JAMA. 2022. PMID: 36125471 Free PMC article. Clinical Trial.
-
Low incidence of late-onset giant cell arteritis during the first year in patients with polymyalgia rheumatica-a repeated imaging study.Rheumatology (Oxford). 2025 Apr 1;64(4):2193-2198. doi: 10.1093/rheumatology/keae463. Rheumatology (Oxford). 2025. PMID: 39180419
-
Polymyalgia Rheumatica and Giant Cell Arteritis: A Systematic Review.JAMA. 2016 Jun 14;315(22):2442-58. doi: 10.1001/jama.2016.5444. JAMA. 2016. PMID: 27299619
References
-
- Buttgereit F, Dejaco C, Matteson EL, Dasgupta B. Polymyalgia rheumatica and giant cell arteritis: A systematic review. JAMA. 2016;315(22):2442–58. - PubMed
-
- Sharma A, Mohammad AJ, Turesson C. Incidence and prevalence of giant cell arteritis and polymyalgia rheumatica: A systematic literature review. Semin Arthritis Rheum. 2020;50(5):1040–8. - PubMed
-
- Dejaco C, Duftner C, Buttgereit F, Matteson EL, Dasgupta B. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology (Oxford). 2017;56(4):506–15. - PubMed
-
- Nielsen AW, Frolund LL, Vaben C, Bonde AR, Gormsen LC, de Thurah AL, et al. Concurrent baseline diagnosis of giant cell arteritis and polymyalgia rheumatica - A systematic review and meta-analysis. Semin Arthritis Rheum. 2022;56:152069. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
