

Remnant cholesterol in early pregnancy as a predictor of gestational diabetes mellitus beyond triglyceride levels: a retrospective cohort study
- PMID: 40691788
- PMCID: PMC12278675
- DOI: 10.1186/s12884-025-07871-y
Remnant cholesterol in early pregnancy as a predictor of gestational diabetes mellitus beyond triglyceride levels: a retrospective cohort study
Abstract
Background: Recent findings suggest remnant cholesterol (RC) may contribute to gestational diabetes mellitus (GDM). This study aimed to explore the link between RC and GDM in early pregnancy to assess RC's risk independently of triglycerides (TG).
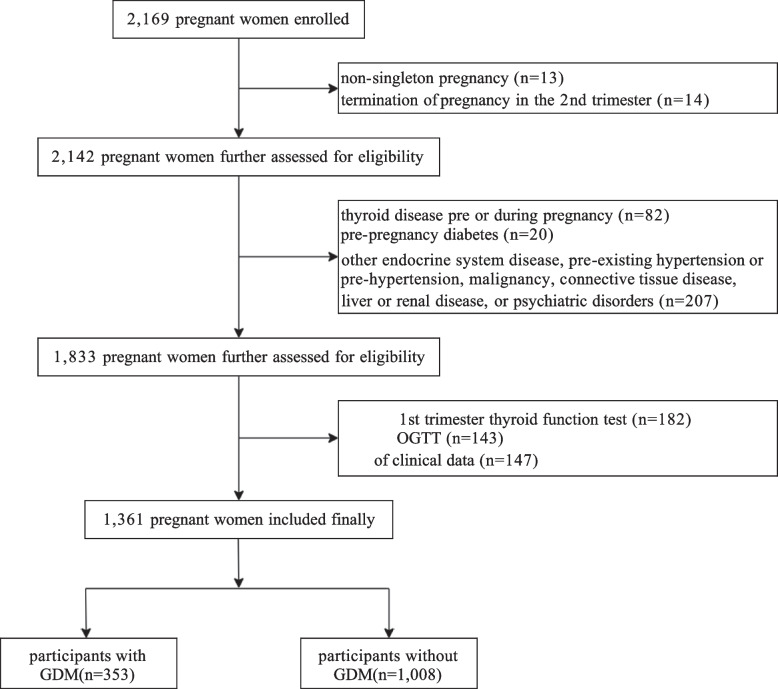
Methods: We performed a retrospective cohort study involving pregnant women admitted to the Suzhou Ninth Hospital affiliated to Soochow University. Data were obtained from the electronic medical record system. RC (mg/dL) was determined by subtracting high-density lipoprotein cholesterol and low-density lipoprotein cholesterol from total cholesterol. GDM was diagnosed using a 75-g oral glucose tolerance test diagnosed at 24-28 weeks of pregnancy. Various analyses, including logistic regressions, restricted cubic spline (RCS), subgroup, sensitivity, and receiver operating characteristic (ROC) analyses, were performed to evaluate the independent association between RC levels and GDM. We conducted discordance analyses to assess GDM risk in RC versus TG discordant and concordant groups using various cut points. The link between RC and different GDM subtypes was also further examined.
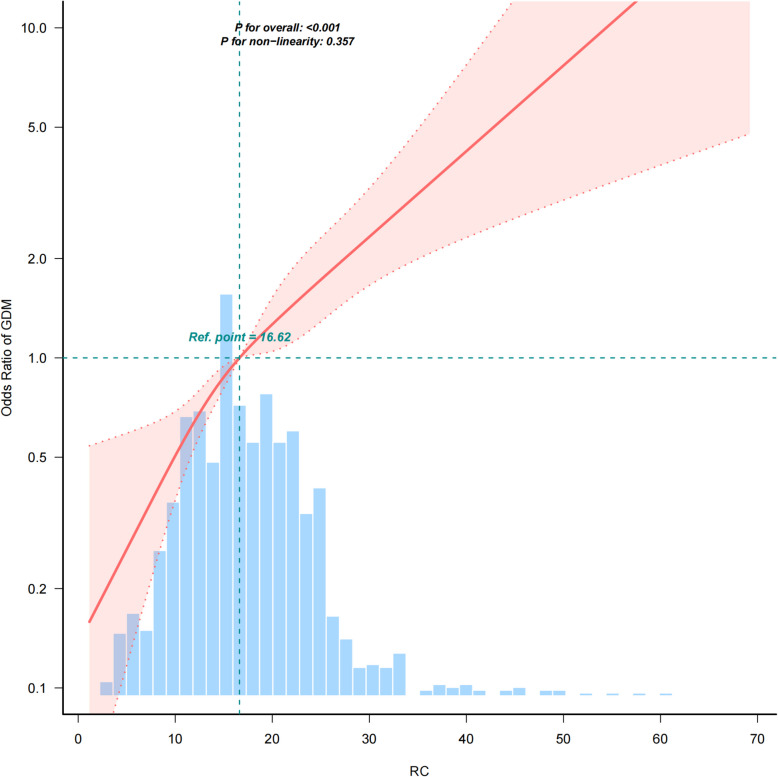
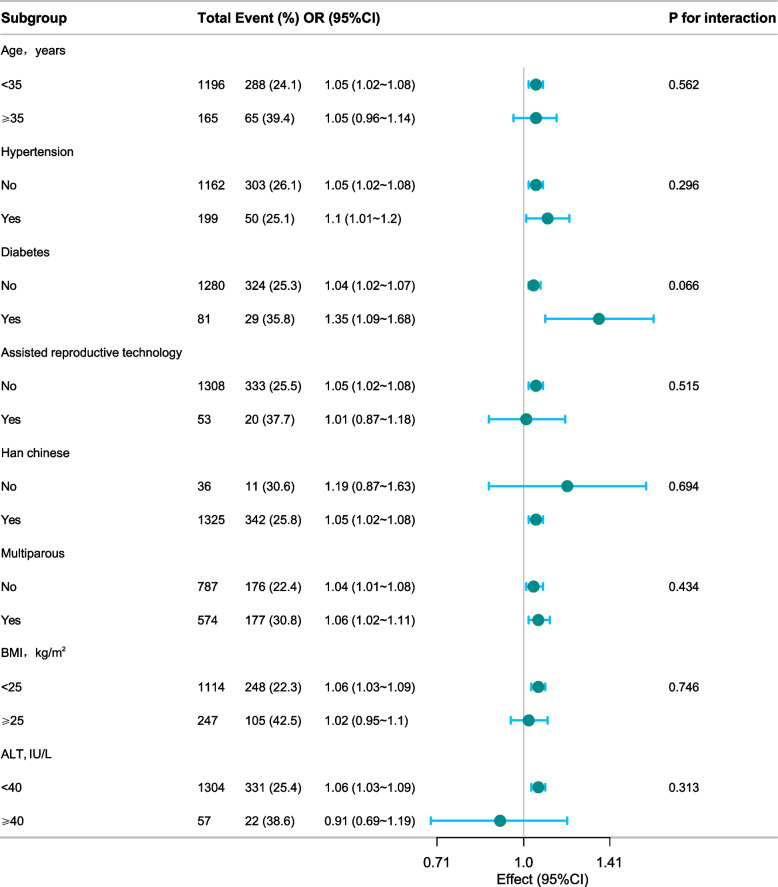
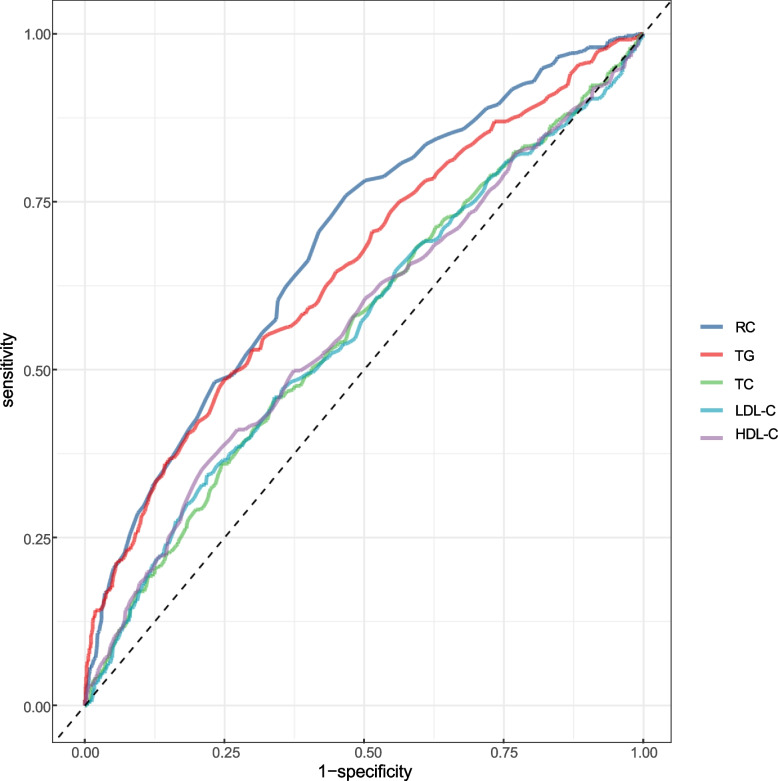
Results: Of the 1,361 women studied, 353 (25.9%) developed GDM. After adjusting for multiple variables, RC was linked to a higher risk of GDM, with an odds ratio (OR) of 1.05 and a 95% confidence interval (CI) of 1.02-1.08. Individuals in the highest RC quartile were more likely to develop GDM (OR: 2.27, 95% CI: 1.37-3.74) than those in the lower quartile. Additionally, the adjusted RCS analysis revealed a significant linear-dose-response link between RC and GDM risk (P for all < 0.001; P for nonlinear = 0.357). Various sensitivity and subgroup analyses confirmed the robustness of our results. The discordant low TG and high RC group revealed an association with GDM, whereas the high TG and low RC group did not when compared with the low TG and low RC group. Even after adjusting for variables, the association remained significant. Similar results were observed using varying clinical cut points. In early pregnancy, RC emerged as the strongest diagnostic marker for GDM, with an ROC curve area of 0.687, surpassing other traditional lipid markers. Further analysis revealed a strong connection between early pregnancy RC levels and GDM subtypes marked solely by high fasting glucose.
Conclusions: Higher RC levels were linked to GDM independently of traditional risk factors, especially TG levels, and may be more useful in diagnosing specific GDM subtypes.
Keywords: Gestational diabetes mellitus; Remnant cholesterol; Triglycerides.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted early at Suzhou Ninth People’s Hospital, affiliated to Soochow University, and was reviewed by the hospital's ethics committee (LOT: KY2022-027–01). All procedures were performed in compliance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
The mediating role of inflammation-related indicators in the association of remnant cholesterol with gestational diabetes mellitus.J Glob Health. 2025 Jun 20;15:04172. doi: 10.7189/jogh.15.04172. J Glob Health. 2025. PMID: 40537057 Free PMC article.
-
First trimester hepatic steatosis index as a predictor of gestational diabetes mellitus: a cohort study in Northwestern China.Sci Rep. 2025 Jul 1;15(1):20975. doi: 10.1038/s41598-025-04510-6. Sci Rep. 2025. PMID: 40595842 Free PMC article.
-
Different strategies for diagnosing gestational diabetes to improve maternal and infant health.Cochrane Database Syst Rev. 2017 Aug 23;8(8):CD007122. doi: 10.1002/14651858.CD007122.pub4. Cochrane Database Syst Rev. 2017. PMID: 28832911 Free PMC article.
-
Different intensities of glycaemic control for women with gestational diabetes mellitus.Cochrane Database Syst Rev. 2016 Apr 7;4(4):CD011624. doi: 10.1002/14651858.CD011624.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2023 Oct 10;10:CD011624. doi: 10.1002/14651858.CD011624.pub3. PMID: 27055233 Free PMC article. Updated.
-
Associations between maternal visceral fat in mid-pregnancy and subsequent gestational diabetes mellitus in a Chinese population: a cohort study.BMC Pregnancy Childbirth. 2025 Jul 10;25(1):746. doi: 10.1186/s12884-025-07873-w. BMC Pregnancy Childbirth. 2025. PMID: 40640737 Free PMC article.
References
-
- ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstet Gynecol. 2018;131:e49-64. - PubMed
-
- Damm P, Houshmand-Oeregaard A, Kelstrup L, Lauenborg J, Mathiesen ER, Clausen TD. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia. 2016;59:1396–9. - PubMed
-
- Simmons D, Immanuel J, Hague WM, Teede H, Nolan CJ, Peek MJ, et al. Treatment of gestational diabetes mellitus diagnosed early in pregnancy. N Engl J Med. 2023;388:2132–44. - PubMed
MeSH terms
Substances
Grants and funding
- WWK202212/the Science, Education, and Health Project in Wujiang District, Suzhou, China
- YK202205/the Project of Suzhou Ninth People's Hospital
- YK202425/the Project of Suzhou Ninth People's Hospital
- 2021YFC2500600, 2021YFC2500602/the Key Programmes of the National Key R&D Program of China
- 8247022695/the National Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
