

Comparison of short-term clinical outcomes and muscle injury in patients with lumbar spinal stenosis undergoing arthroscopic-assisted uni-portal spinal surgery, unilateral biportal endoscopic surgery, and percutaneous interlaminar lumbar discectomy: a six-month follow-up
- PMID: 40691813
- PMCID: PMC12278621
- DOI: 10.1186/s13018-025-06088-1
Comparison of short-term clinical outcomes and muscle injury in patients with lumbar spinal stenosis undergoing arthroscopic-assisted uni-portal spinal surgery, unilateral biportal endoscopic surgery, and percutaneous interlaminar lumbar discectomy: a six-month follow-up
Abstract
Objective: This study aims to assess and compare the six-month postoperative clinical outcomes of Arthroscopic-assisted Uni-portal Spinal Surgery (AUSS), unilateral biportal endoscopy (UBE), and percutaneous interlaminar endoscopic discectomy (PEID) for lumbar spinal stenosis (LSS). Additionally, muscle injury associated with these procedures is evaluated by analyzing changes in creatine kinase (CK) and C-reactive protein (CRP) levels.
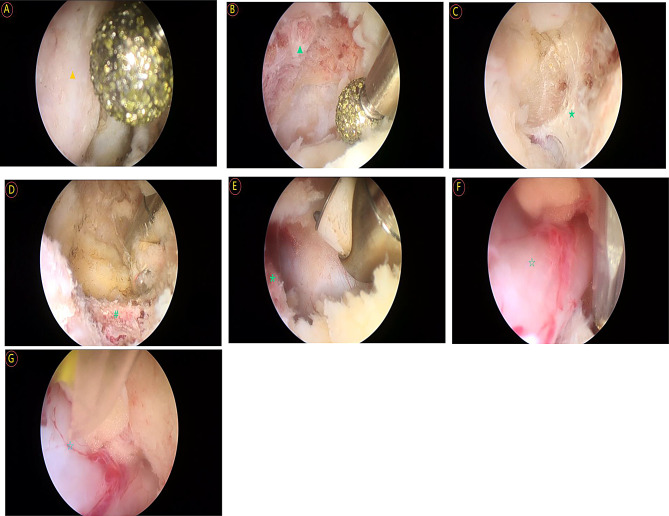
Methods: A total of 288 patients diagnosed with single-segment unilateral LSS and treated between January 2021 and June 2024 were included in this study. Patients were assigned to the AUSS group (n = 129), UBE group (n = 86), or PEID group (n = 73). Surgical parameters, including operative time, incision length, intraoperative blood loss, and postoperative facet joint preservation rate, were recorded. Clinical outcomes were assessed preoperatively and at 3 days, 3 months, and 6 months postoperatively using the Visual Analog Scale (VAS) for back and leg pain, Oswestry Disability Index (ODI), EQ-5D-5 L quality of life index, and the modified Macnab criteria. The extent of muscle injury was quantified through serum CK and CRP levels measured preoperatively and on postoperative days 1, 3, 5, and 7. Descriptive statistics and multiple comparison analyses were used to assess clinical parameters among the three groups. Longitudinal data were analyzed using a generalized mixed linear model.
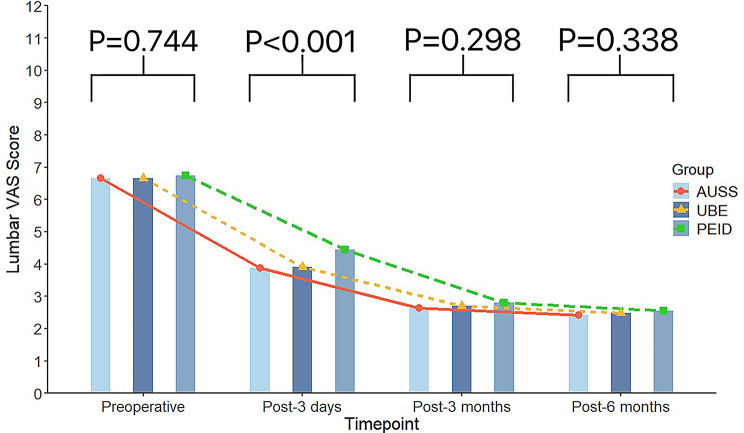
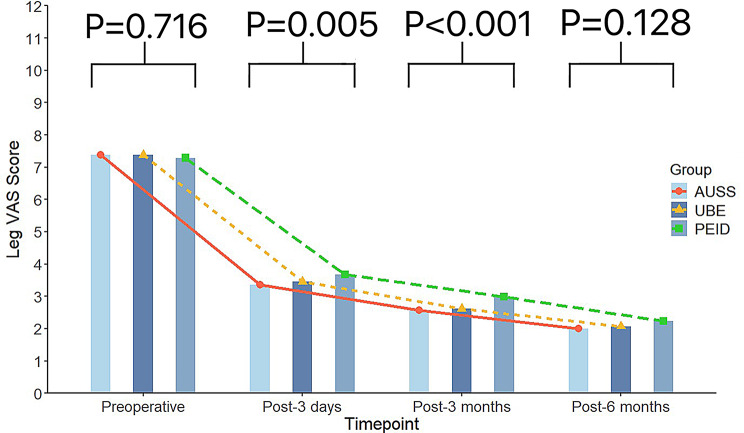
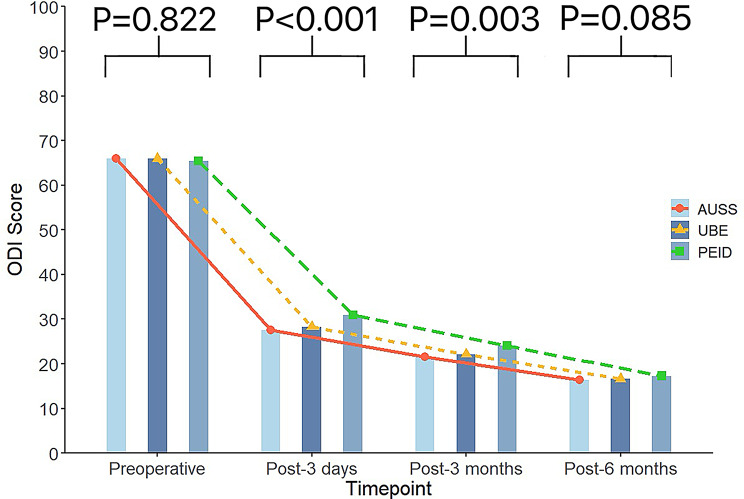
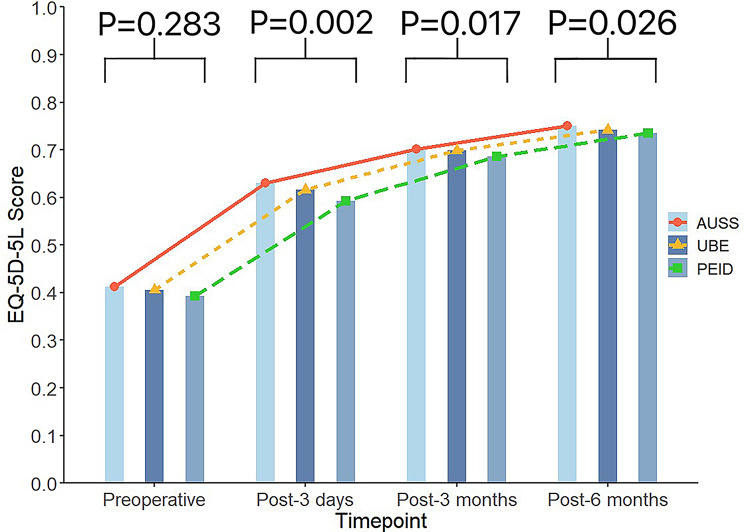
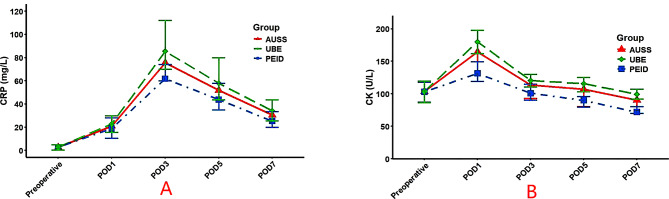
Results: The AUSS group demonstrated significantly shorter operative times and smaller incision lengths compared to the UBE and PEID groups (P < 0.001). Postoperative VAS scores decreased significantly in all three groups, with the greatest improvement observed in the AUSS group (P < 0.05). ODI and EQ-5D-5 L scores indicated superior postoperative quality of life in the AUSS group compared to the UBE and PEID groups (P < 0.05). However, no statistically significant differences were observed in the modified Macnab criteria outcomes or postoperative complication rates among the three groups (P > 0.05). The PEID group exhibited the lowest postoperative CK and CRP levels as well as the least intraoperative blood loss (P < 0.05), suggesting minimal muscle injury. The AUSS group showed lower muscle injury levels than the UBE group (P < 0.05).
Conclusion: Arthroscopic-assisted Uni-portal Spinal Surgery (AUSS), unilateral biportal endoscopic (UBE) technique, and percutaneous endoscopic interlaminar discectomy (PEID) are all effective minimally invasive approaches for lumbar spinal stenosis (LSS). AUSS offers shorter operative time and better preservation of anatomical structures. PEID minimizes intraoperative tissue damage and reduces inflammatory response, while UBE balances visualization with operational flexibility. All three techniques demonstrate good short-term clinical outcomes. The surgical approach should be tailored to each patient's symptoms and individualized needs. Although AUSS demonstrated certain intraoperative advantages, this study did not show that AUSS is superior to UBE or PEID in clinical efficacy or complication control. As a novel technique, AUSS may improve postoperative pain and quality of life, providing a valuable addition to the minimally invasive treatment options for lumbar spinal stenosis.
Keywords: Arthroscopic-assisted uni-portal spinal surgery; Lumbar spinal stenosis; Percutaneous interlaminar endoscopic discectomy; Unilateral biportal endoscopy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: All procedures were conducted in accordance with the ethical standards of the institutional and/or national research committees. This study was approved by the Ethics Committee of Qinghai Red Cross Hospital (KY-2024-60). Informed consent was obtained from all patients. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Unilateral biportal endoscopic discectomy versus percutaneous endoscopic lumbar discectomy in the treatment of far-lateral lumbar disc herniation.Neurosurg Rev. 2025 Aug 4;48(1):588. doi: 10.1007/s10143-025-03748-y. Neurosurg Rev. 2025. PMID: 40758136
-
Unilateral biportal endoscopic versus microscopic discectomy in degenerative lumbar spinal stenosis: A prospective cohort study.Medicine (Baltimore). 2025 May 23;104(21):e42594. doi: 10.1097/MD.0000000000042594. Medicine (Baltimore). 2025. PMID: 40419907 Free PMC article. Clinical Trial.
-
Comparison of surgical invasiveness and hidden blood loss between unilateral double portal endoscopic lumbar disc extraction and percutaneous endoscopic interlaminar discectomy for lumbar spinal stenosis.J Orthop Surg Res. 2024 Nov 21;19(1):778. doi: 10.1186/s13018-024-05274-x. J Orthop Surg Res. 2024. PMID: 39567947 Free PMC article.
-
Clinical outcomes of uniportal compared with biportal endoscopic decompression for the treatment of lumbar spinal stenosis: a systematic review and meta-analysis.Eur Spine J. 2023 Aug;32(8):2717-2725. doi: 10.1007/s00586-023-07660-1. Epub 2023 Mar 29. Eur Spine J. 2023. PMID: 36991184
-
Surgical options for lumbar spinal stenosis.Cochrane Database Syst Rev. 2016 Nov 1;11(11):CD012421. doi: 10.1002/14651858.CD012421. Cochrane Database Syst Rev. 2016. PMID: 27801521 Free PMC article.
References
-
- Costa F, Sassi M, Cardia A, Ortolina A, De Santis A, Luccarell G, et al. Degenerative lumbar spinal stenosis: analysis of results in a series of 374 patients treated with unilateral laminotomy for bilateral microdecompression. J Neurosurgery: Spine. 2007;7(6):579–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
