

Readiness and leadership for the implementation of polygenic risk scores: Genetic healthcare providers' perspectives in the hereditary cancer context
- PMID: 40692272
- PMCID: PMC12280534
- DOI: 10.1002/jgc4.70084
Readiness and leadership for the implementation of polygenic risk scores: Genetic healthcare providers' perspectives in the hereditary cancer context
Abstract
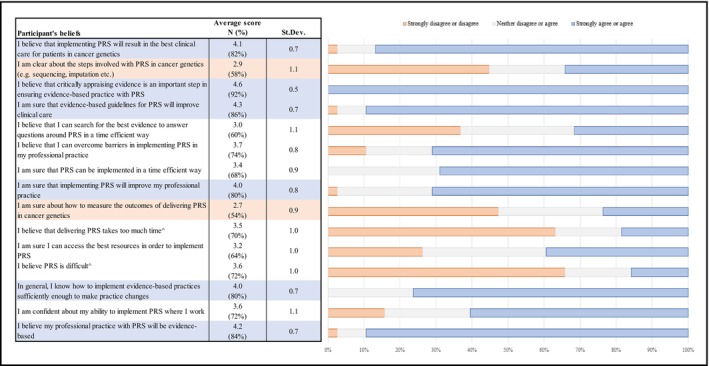
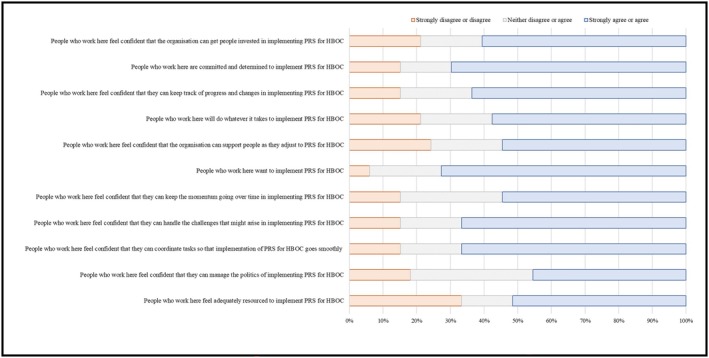
Genetic healthcare providers and organizations must be made ready for potential future clinical implementation of polygenic risk scores (PRS) for hereditary breast and ovarian (HBOC) cancer risk assessment. Understanding the multi-level factors that contribute to readiness for change will assist leaders with strategic planning and selection of facilitative implementation strategies, ultimately reducing resource wastage and increasing the likelihood of implementation success. Evidence is missing on the current state of readiness in the Australian cancer genomics sector. The aim of this study was to explore genetic healthcare providers' perspectives on organizational readiness and leadership. Participants were recruited through professional networks to complete an online, quantitative survey encompassing multiple validated evidence-based tools. Analyses included descriptive and inferential statistics. Participants (N = 40) were majority female (N = 31, 77.5%) and in clinical roles (N = 31, 77.5%). A high level of personal capability and organizational readiness was found, with current workplace behaviors and culture being enablers for implementation. Barriers to readiness were knowledge of implementation and evaluative processes for PRS and insufficient resourcing. Leaders were confident in their roles and supportive and perseverant behaviors. Participants in non-leadership roles regarded leadership at an average level. Overall, leadership proactivity toward implementation of PRS for HBOC risk assessment was low. If implementation is to be successful, investment in further developing organizational climates conducive to change is required, focusing on interventions to bolster entrepreneurial leadership behaviors and increase implementation competency and resourcing. Further research into readiness and leadership in clinical cancer genetics is needed.
Keywords: hereditary breast and ovarian cancer risk assessment; implementation; leadership; organizational readiness; polygenic risk scores.
© 2025 The Author(s). Journal of Genetic Counseling published by Wiley Periodicals LLC on behalf of National Society of Genetic Counselors.
Conflict of interest statement
Ms. Rebecca Purvis, Associate Professor Natalie Taylor, Ms. Mary‐Anne Young, Professor Paul James, and Associate Professor Laura E. Forrest all declare no conflicts of interest.
Figures
References
-
- Aarons, G. A. , Ehrhart, M. G. , Farahnak, L. R. , Sklar, M. , & Horowitz, J. (2017). Discrepancies in leader and follower ratings of transformational leadership: Relationships with organizational culture in mental health. Administration and Policy in Mental Health and Mental Health Services Research, 44(4), 12. - PMC - PubMed
-
- Albers, B. , Shlonsky, A. , & Mildon, R. (2020). Implementation science 3.0. Springer Nature Switzerland AG.
MeSH terms
LinkOut - more resources
Full Text Sources
