

Cardiofaciocutaneous syndrome and immunodeficiency: data from an international multicenter cohort
- PMID: 40692796
- PMCID: PMC12277328
- DOI: 10.3389/fimmu.2025.1598896
Cardiofaciocutaneous syndrome and immunodeficiency: data from an international multicenter cohort
Abstract
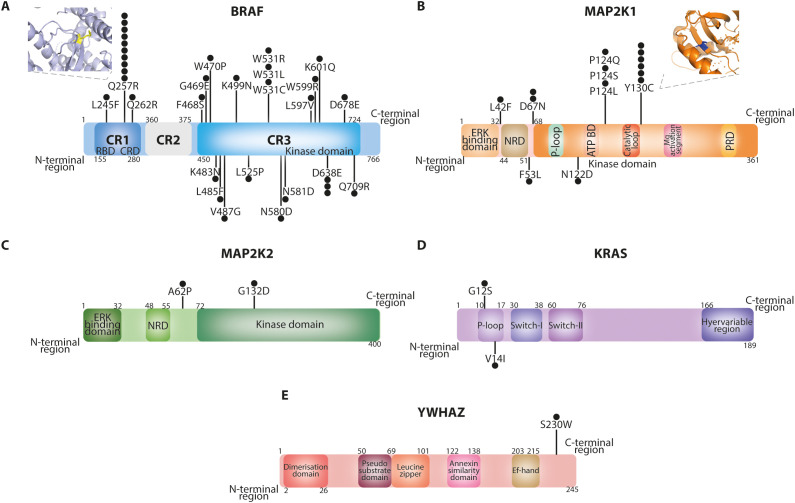
Introduction: Cardiofaciocutaneous syndrome (CFCS) is a rare syndromic disorder caused by germline mutations affecting the RAS/MAPK pathway. It is characterized by distinctive craniofacial dysmorphism, congenital heart defects, skin abnormalities, gastrointestinal dysfunction, neurocognitive impairment, and epilepsy. Emerging evidence suggests an association with hypogammaglobulinemia, but a comprehensive characterization of immunological abnormalities in CFCS is lacking.
Methods: We conducted a retrospective, multicenter observational study to investigate the immunological phenotype of CFCS. Clinical features, immune-related manifestations, and laboratory parameters were analyzed to delineate the immunological profile of affected individuals.
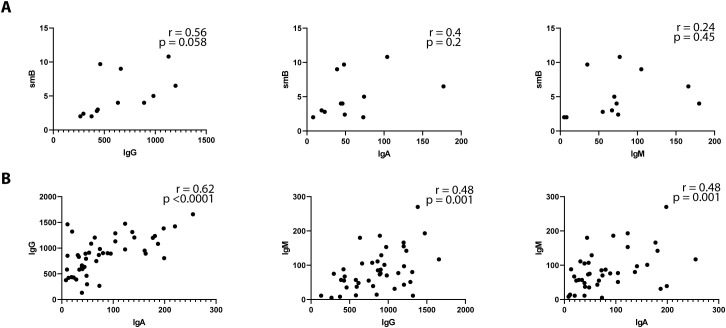
Results: A total of 56 patients with a confirmed clinical and molecular diagnosis of CFCS were included, with a median age at evaluation of 13 years (range: 1-39 years). Increased susceptibility to infections was reported in 18/56 patients (32%), while autoimmune manifestations were observed in 14/56 patients (25%). Common immunological findings included monocytosis (32%), lymphopenia (21%), and hypogammaglobulinemia, with decreased IgG, IgA, or IgM levels in 21%, 40%, and 35% of patients, respectively. Genotype-phenotype analysis revealed that BRAF mutations were predominantly associated with T-cell lymphopenia, whereas MAP2K1 mutations were linked to monocytosis, reduced naïve and switched-memory B cells, and hypogammaglobulinemia. Immunodeficiency-related treatments, including immunoglobulin replacement therapy, antibiotic prophylaxis, or immunosuppressive therapy, were administered to 6/56 patients (11%).
Conclusions: CFCS is associated with recurrent yet heterogeneous immunological abnormalities, including lymphopenia, hypogammaglobulinemia, and increased infection susceptibility. Given these findings, routine immunological assessment should be considered in CFCS patients to facilitate early detection and appropriate management of immune dysfunction.
Keywords: BRAF; MAP2K1; Syndromic immunodeficiency; cardiofaciocutaneous syndrome; hypogammaglobulinemia; inborn errors of immunity; primary immunodeficiency; rasopathy.
Copyright © 2025 Di Majo, Leoni, Cartisano, Fossati, Viscogliosi, Trevisan, Bruno, Conti, Moratti, Monaco, Rigante, Rivalta, Cancrini, Szczawińska-Popłonyk, Jamsheer, Obara-Moszyńska, Zakharova, Shcherbina, Rodina, Tüysüz, Jamuar, Lim, Goh, Cereda, Agovino, Contaldo, Gambardella, Balduzzi, Cherubino, Marrocco, Bellesi, Carusi, Rumi, Biondi, Zampino and Saettini.
Conflict of interest statement
AJ was employed by Diagnostyka GENESIS. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Characterisation of Challenging Behaviours and Associated Genetic and Neurological Features in Cardiofaciocutaneous Syndrome.J Intellect Disabil Res. 2025 Aug;69(8):682-692. doi: 10.1111/jir.13247. Epub 2025 May 19. J Intellect Disabil Res. 2025. PMID: 40387217 Free PMC article.
-
Epilepsy and BRAF Mutations: Phenotypes, Natural History and Genotype-Phenotype Correlations.Genes (Basel). 2021 Aug 26;12(9):1316. doi: 10.3390/genes12091316. Genes (Basel). 2021. PMID: 34573299 Free PMC article.
-
A literature review and pooled case analysis of cardiofaciocutaneous syndrome to estimate cancer risk.Genet Med. 2025 Jul;27(7):101423. doi: 10.1016/j.gim.2025.101423. Epub 2025 Apr 4. Genet Med. 2025. PMID: 40196938 Review.
-
Dermoscopic Features of Melanocytic Nevi in Cardiofaciocutaneous and Costello Syndromes.JAMA Dermatol. 2024 Aug 1;160(8):869-873. doi: 10.1001/jamadermatol.2024.1697. JAMA Dermatol. 2024. PMID: 38888893 Free PMC article.
-
[Cardiofaciocutaneous syndrome caused by microdeletion of chromosome 19p13.3: a case report and literature review].Zhongguo Dang Dai Er Ke Za Zhi. 2025 Jul 15;27(7):854-858. doi: 10.7499/j.issn.1008-8830.2502003. Zhongguo Dang Dai Er Ke Za Zhi. 2025. PMID: 40695519 Free PMC article. Review. Chinese.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous