

PILOT STUDY OF COMBINED TRANSVERTEBRAL MAGNETIC AND TRANSCUTANEOUS STIMULATION FOR THE REHABILITATION OF COMBAT ACUTE SPINAL CORD INJURIES
- PMID: 40692816
- PMCID: PMC12278770
- DOI: 10.2340/jrm-cc.v8.42686
PILOT STUDY OF COMBINED TRANSVERTEBRAL MAGNETIC AND TRANSCUTANEOUS STIMULATION FOR THE REHABILITATION OF COMBAT ACUTE SPINAL CORD INJURIES
Abstract
Aim of the study: To improve the effectiveness of neurorehabilitation in patients with severe combat spinal cord injury by combining spinal cord repetitive transvertebral magnetic stimulation (rTvMS) and non-invasive transcutaneous electrical stimulation (TcES) of peripheral nerves.
Clinical rationale for study: For the best recovery from severe combat spinal cord injury, neurorehabilitation must start in the acute phase. Only technologies targeting sensorimotor conduction and functional improvement can confirm the potential of the time factor. Non-invasive neuromodulation has been shown to work for combat spinal cord injury of varying severity.
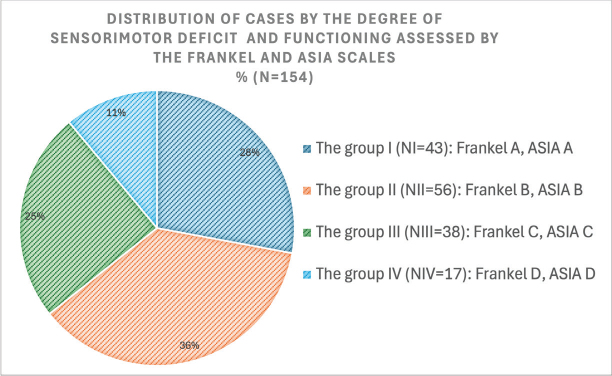
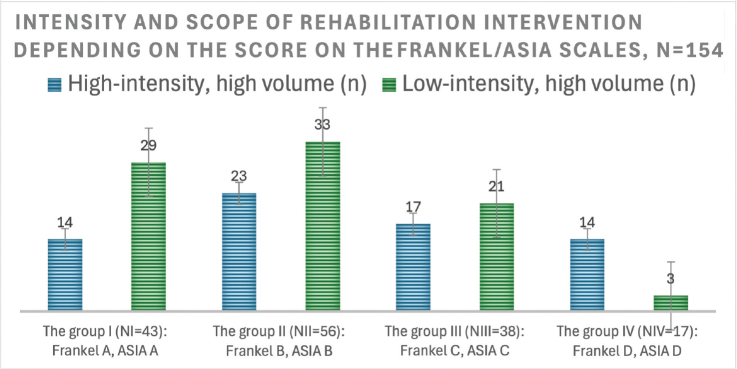
Material and methods: We have analysed 154 cases of severe combat spinal cord injury, followed continuously for at least 12 months from the start of neurorehabilitation. A unified «end-to-end» protocol combined rTvMS of the spinal cord with simultaneous TcES of peripheral nerves in different modes was developed for non-invasive spinal cord neuromodulation.
Results: The combination of these parameters produced the most positive results in post-traumatic sensory-motor disorders: (i). rTvMS, level ThX-LI: 2000 pulses per set, 100 pulse packages, 5-10 Hz, intensity "+ 30--40%" of the threshold of the evoked motor potential; TcES n. tibialis or n. peroneus: 5-10 Hz, pulse intensity corresponded to the threshold of the motor response, functional electrical stimulation (FES) mode. (ii). rTvMS, level CII-ThII: 2000 pulses per set, 50 pulse packages, 5-7 Hz, intensity + 20-30% of the threshold of the evoked motor potential; TcES n. medianus or n. ulnaris; n. tibialis or n. peroneus: 5-10 Hz, pulse intensity corresponded to the threshold of the motor response, FES mode. Approximately 28% of patients in group A (FRANKEL/ASIA) moved to a higher level of function after 3 courses of neurorehabilitation intervention (90 working days).
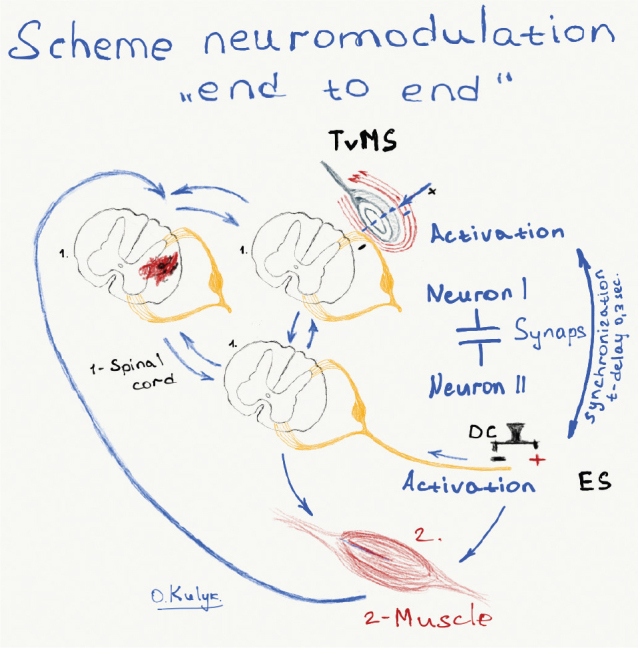
Conclusions and clinical implications: Electro-magnetic stimulation of the spinal cord excitatory cell conduction system according to the principle of "end-to-end: as in Hebb's theory," combined with physical movement, led to an increase in spinal cord conduction in the acute phase of combat spinal cord injury. This was manifested by neurological and functional improvement.
Keywords: combating spinal cord injury; early neurorehabilitation; non-invasive electrical stimulation of peripheral nerves; transvertebral magnetic stimulation for spinal cord injury.
Plain language summary
If you imagine, for example, that the ability to move a person’s legs or arms depends on 2 nerve cells that are connected and form a kind of conductor or bridge, the ends of which are these cells, then any physical impact that breaks this contact will lead to the loss of this ability. Now, if we imagine that for every cell that has lost contact with another, we act in such a way that, under the influence of this action, they re-establish this connection; it is evident that this can lead to the restoration of movement. It is this «end-to-end» effect, that is simultaneously from both ends with electromagnetic waves of specific parameters on spinal cord cells above and below the level of damage, in combination with specific physical exercises, that led to the improvement of motor and sensory functions after severe gunshot spinal cord injury.
© 2025 The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

Similar articles
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Short-Term Memory Impairment.2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Jun 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31424720 Free Books & Documents.
-
Management of faecal incontinence and constipation in adults with central neurological diseases.Cochrane Database Syst Rev. 2013 Dec 18;(12):CD002115. doi: 10.1002/14651858.CD002115.pub4. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2014 Jan 13;(1):CD002115. doi: 10.1002/14651858.CD002115.pub5. PMID: 24347087 Updated.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
-
- Kulyk OV. The method of rehabilitation of patients with functional disorders and the effects of focal lesions of the central and peripheral nervous system. Patent of Ukraine No. 67557. 2012. State Intellectual Property Service (Ukrainian Patent Office), Ukriane.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
