

Deupirfenidone (LYT-100) in post-acute sequelae of SARS-CoV-2 with respiratory complications
- PMID: 40692836
- PMCID: PMC12278312
- DOI: 10.1183/23120541.01142-2024
Deupirfenidone (LYT-100) in post-acute sequelae of SARS-CoV-2 with respiratory complications
Abstract
Introduction: The pathophysiology of respiratory complications in post-acute sequelae of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection (PASC) is poorly understood, but a high incidence of progressive pulmonary fibrosis was anticipated. Deupirfenidone (LYT-100) is a selectively deuterated form of pirfenidone that retains antifibrotic and anti-inflammatory activity but with improved tolerability. This study evaluated the safety and efficacy of deupirfenidone in PASC patients with respiratory complications.
Methods: Global, double-blind, randomised placebo-controlled trial evaluating 750 mg deupirfenidone twice daily versus placebo for 3 months in PASC patients with respiratory complications following hospitalisation for acute COVID-19 infection severe enough to necessitate supplemental oxygen (NCT04652518).
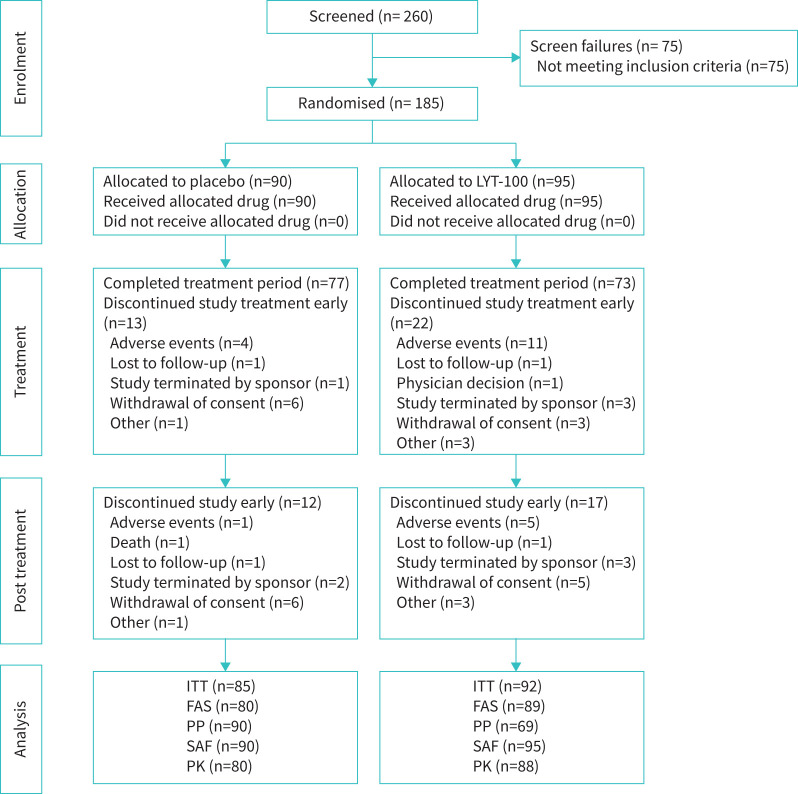
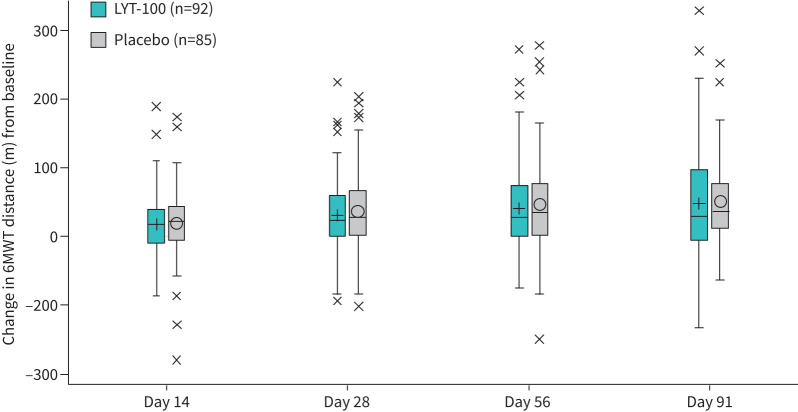
Results: 185 patients were randomised and treated (95 with deupirfenidone, 90 with placebo), with 177 included in the modified intention-to-treat population. The mean age was 54.5 years, 62.7% were male and 10.7% had prior mechanical ventilation. The 6-min walk distance improved across both arms between baseline and day 91 (deupirfenidone 44.3 m (95% CI 24.8-63.8 m) versus placebo 48.8 m (95% CI 29.2-68.4 m); p=0.70). The most common treatment-emergent adverse events (TEAEs) for deupirfenidone versus placebo were nausea (9.5% versus 1.1%), upper abdominal discomfort (5.3% versus 2.2%) and dyspepsia (6.3% versus 1.1%). TEAEs leading to trial drug discontinuation were 11.6% for deupirfenidone and 4.4% for placebo. The proportion of discontinuations considered at least possibly related to treatment was 8.6% for deupirfenidone and 2.4% for placebo.
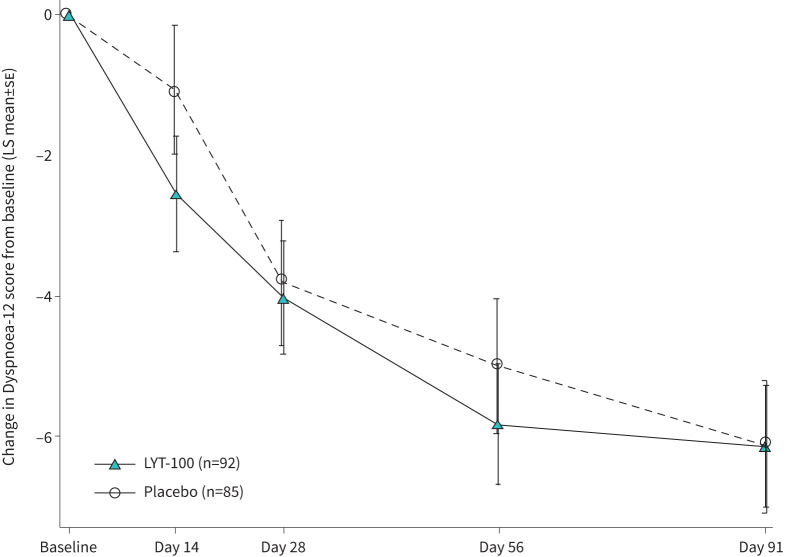
Discussion: Most patients with PASC and respiratory complications showed significant improvement over 91 days irrespective of treatment assignment. Deupirfenidone was well tolerated, with low rates of TEAEs, which supports further investigation in patients with idiopathic pulmonary fibrosis.
Copyright ©The authors 2025.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous