

Forearm fractures treated with elastic stable intramedullary nailing: Is casting still necessary?
- PMID: 40692964
- PMCID: PMC12276208
- DOI: 10.1177/18632521251352323
Forearm fractures treated with elastic stable intramedullary nailing: Is casting still necessary?
Abstract
Introduction: Elastic stable intramedullary nailing is widely recognized for treating pediatric forearm fractures due to its stable fixation and minimal impact on soft tissue. Traditionally, casting has followed elastic stable intramedullary nailing; however, recent studies question its necessity. This study evaluates the outcomes of omitting casts post-elastic stable intramedullary nailing, examining healing speed and quality of life compared to cases where casting was applied.
Materials and methods: A prospective study was conducted from 2022 to 2024 in an urban hospital, where children with both-bone midshaft forearm fracture were randomized to receive or not receive casting after elastic stable intramedullary nailing. Age- and sex-matched patients were selected to allow for accurate comparison. The study included patients aged 5 to 14 years. Outcomes were measured using radiographic scores and quality-of-life assessments.
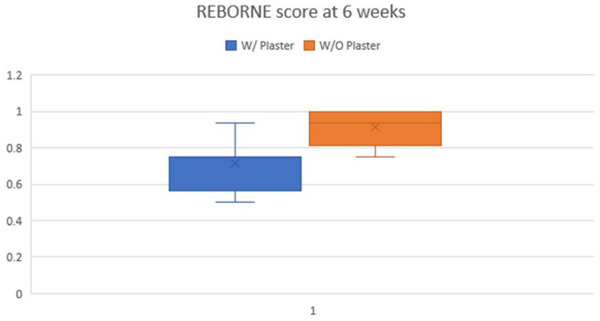
Results: From a total of 355 patients, 136 cases were included in the assessment. Analysis indicated faster healing in patients without postoperative casting, as evidenced by higher REBORNE scores at 3 weeks and 2 months. Quality of life, measured by the Pediatric Quality of Life Inventory, was also significantly improved in the no-cast group at 6 weeks.
Discussion: Our findings suggest that elastic stable intramedullary nailing provides sufficient stability for both-bone midshaft forearm fracture, making additional casting unnecessary. Early mobilization led to better functional outcomes without increasing complications. Although some minor early discomfort was reported, the cast-free approach proved effective and safe.
Conclusion: Elastic stable intramedullary nailing remains the gold standard for treating pediatric forearm fractures. Our preliminary results indicate that for both-bone midshaft forearm fracture, elastic stable intramedullary nailing can be safely performed without postoperative casting, promoting faster healing and better patient satisfaction.
Keywords: ESIN; Forearm shaft fractures; both-bone midshaft forearm fracture; casting; children.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures







References
-
- Sinikumpu JJ, Lautamo A, Pokka T, et al. The increasing incidence of paediatric diaphyseal both-bone forearm fractures and their internal fixation during the last decade. Injury 2012; 43(3): 362–366. - PubMed
-
- Kramhøft M, Bødtker S. Epidemiology of distal forearm fractures in Danish children. Acta Orthop Scand 1988; 59(5): 557–559. - PubMed
-
- Alpar EK, Thompson K, Owen R, et al. Midshaft fractures of forearm bones in children. Injury 1981; 13(2): 153–158. - PubMed
-
- Rennie L, Court-Brown CM, Mok JYQ, et al. The epidemiology of fractures in children. Injury 2007; 38(8): 913–922. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous