

Clinical prognostic value of TTV and HCMV but not EBV for outcomes in hospitalized HIV-positive patients
- PMID: 40693040
- PMCID: PMC12276542
- DOI: 10.1016/j.bsheal.2025.05.006
Clinical prognostic value of TTV and HCMV but not EBV for outcomes in hospitalized HIV-positive patients
Abstract
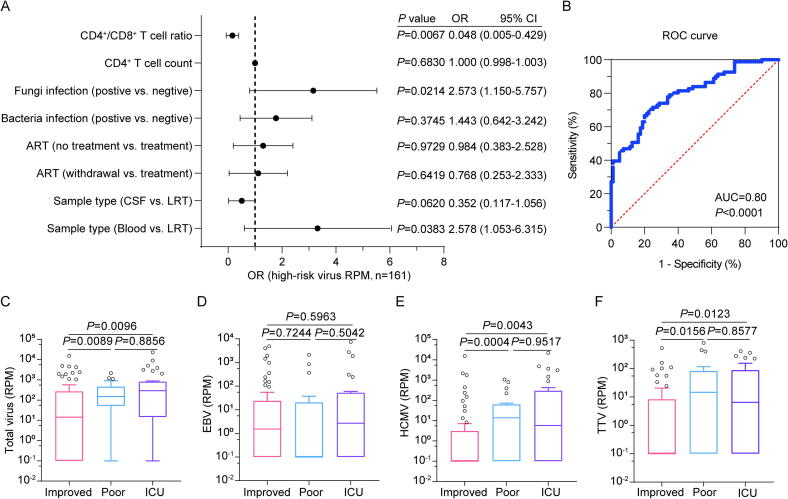
Opportunistic infections caused by viruses, bacteria, fungi, and parasites, are commonly reported in hospitalized human immunodeficiency virus (HIV)-positive patients, but their detrimental contribution to disease severity remains under explored. In this study, we examined the coinfection profiles of 126 HIV-positive patients with suspected respiratory, bloodstream, or neurological infections. Lower respiratory tract (LRT) samples, cerebrospinal fluid, and blood samples collected within the first seven days of admission were subjected to metagenomic next-generation sequencing (mNGS). Additionally, a multiplex polymerase chain reaction (PCR) detection kit to identify ten commonly known respiratory pathogens was applied to the LRT samples. Of 126 HIV-positive patients, 111 (88.1 %) were coinfected with at least one known virus. Epstein-Barr virus (EBV) (71/111, 64.0 %), human cytomegalovirus (HCMV) (64/111, 57.7 %), and torque teno virus (TTV) (63/111, 56.8 %) were the three most prevalent coinfected viruses. Fungal coinfections (58/126, 46.0 %) and bacterial coinfections (47/126, 37.3 %) were less frequent than viral coinfections. Higher viral loads of coinfection were associated with fungal coinfections (odds ratio [OR] = 2.573, 95 % confidence interval [CI]: 1.150-5.757, P = 0.0214) and lower CD4+/CD8+ T cell ratios (OR = 0.048, 95 % CI: 0.005-0.429, P = 0.0067). Importantly, patients with higher loads of HCMV and TTV, but not EBV, exhibited worse clinical outcomes. Specifically, patients with HCMV reads per million (RPM) > 0 and TTV RPM > 5 exhibited significantly higher risks of poor prognosis and intensive care unit (ICU) admission. In contrast, EBV RPM showed no association with clinical outcomes in this context. In conclusion, HCMV and TTV may serve as prognostic biomarkers linked to poorer outcomes in HIV-positive patients. Detection of HCMV and TTV could predict clinical outcomes and improve patient management strategies.
Keywords: Epstein-Barr virus (EBV); Human cytomegalovirus (HCMV); Human immunodeficiency virus (HIV); Pathogen-coinfected profile; Prognostic value; Torque teno virus (TTV).
© 2025 Chinese Medical Association Publishing House. Published by Elsevier B.V.
Figures




References
-
- UNAIDS/WHO, HIV statistics, globally and by WHO region, 2023. https://www.who.int/publications/i/item/WHO-UCN-HHS-SIA-2023-01, 2023 (accessed 17 July 2024).
-
- China Daily, HIV infections in check, but more efforts needed, 2023. https://www.chinadaily.com.cn/a/202312/01/WS6569e692a31090682a5f106a.html, 2023 (accessed 19 September 2024).
LinkOut - more resources
Full Text Sources
Research Materials
