

A Text Message Intervention to Minimize the Time Burden of Cancer Care
- PMID: 40693184
- PMCID: PMC12276887
- DOI: 10.1056/cat.24.0201
A Text Message Intervention to Minimize the Time Burden of Cancer Care
Abstract
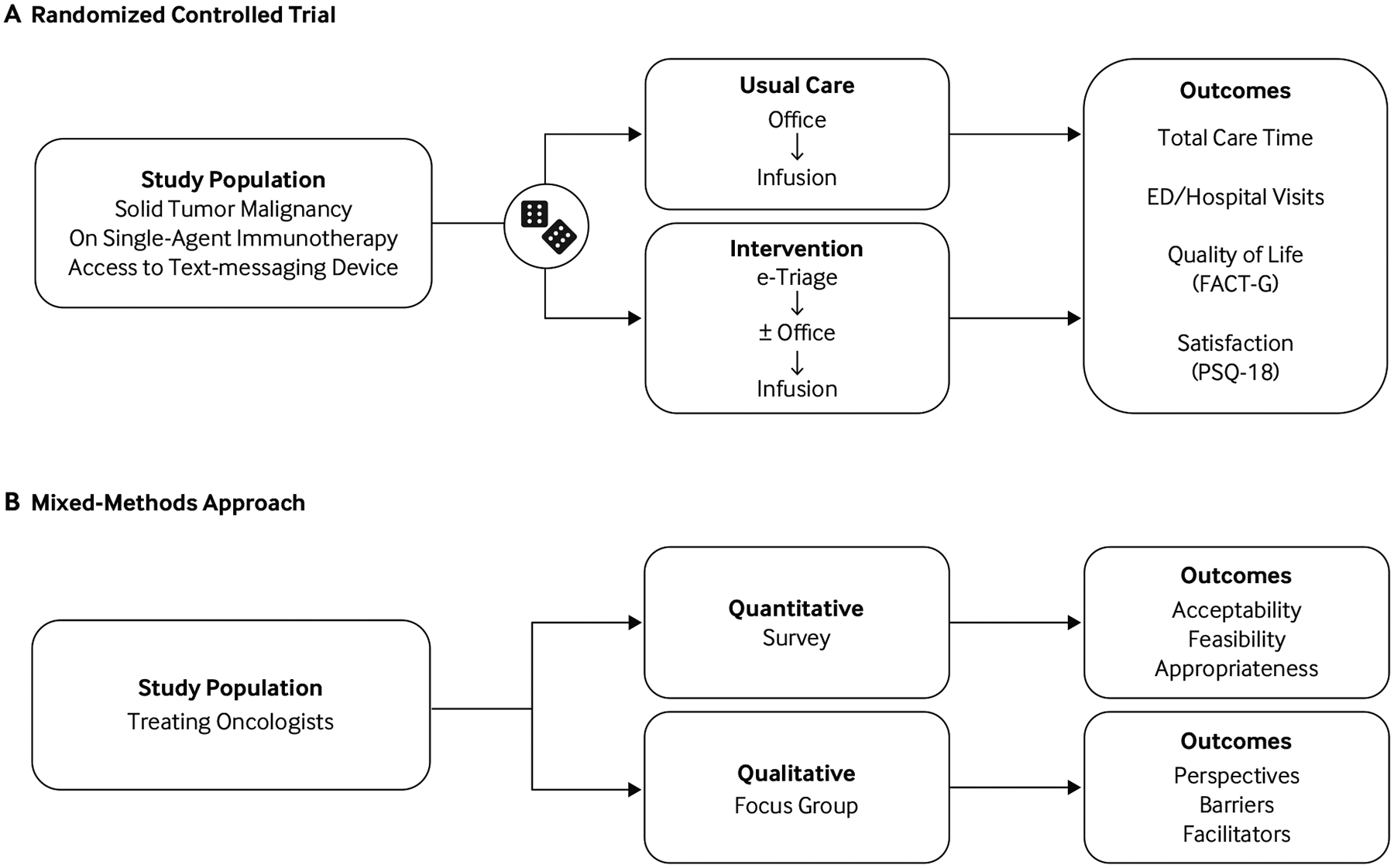
Patients with cancer spend considerable time commuting to, waiting for, and receiving health care. Patient-reported outcomes have been collected electronically to monitor patients for toxicity related to treatment, but, to the authors' knowledge, they have not been used as a strategy to minimize patients' time spent on cancer care by streamlining care delivery. Researchers at Penn Medicine set an objective to assess the effectiveness and implementation of a text message-based symptom reporting electronic triage (e-triage) versus usual care to minimize the time toxicity associated with ambulatory cancer care. The methods employed included a hybrid type 1 effectiveness-implementation, unblinded, randomized controlled trial and sequential mixed-methods study, which was conducted between December 1, 2021, and December 31, 2022, with a follow-up period of 3 months or three visits (whichever came first, but all within the 2-year window). Adult patients with solid tumors receiving single-agent immune checkpoint inhibitors (ICIs) with access to a text-messaging device were enrolled, with a target sample size of 176. The intervention was a symptom-based e-triage via mobile text messaging combined with routine laboratory testing. Participants in the e-triage group with normal bloodwork and no symptoms of drug toxicity on e-triage were eligible to fast-track to ICI infusion, bypassing the pretreatment office visit. The primary end point was total time per ambulatory encounter; secondary end points included wait time, ED or hospital visits, health-related quality of life, patient satisfaction, and implementation (reach and fidelity). Implementation readiness (acceptability, appropriateness, and feasibility), barriers, and facilitators were evaluated in a mixed-methods analysis among treating oncologists, measured via surveys and focus groups. For the study, 40 patients were randomly assigned, of which 31 were evaluated for the primary end point; the median age among the 40 participants was 67.5 years of age (interquartile range 59.5-71.5 years of age), 80.0% were male, and 84.6% were white. Those randomly assigned to the e-triage group of the pilot randomized controlled trial (n=19, n=16 evaluable) had an average of 66.0 minutes less total time (95% confidence interval [CI], -123.7 to -8.08 minutes; P=0.03) and 30.1 minutes less wait time (95% CI, -60.9 to 1.1 minutes; P=0.08) per encounter, than those in usual care (n=21 randomly assigned, n=15 evaluable). ED or hospital visits, health-related quality of life, and patient satisfaction scores were similar. In the mixed-methods study, oncologists (n=31, 17 completed the survey) found the e-triage acceptable (mean 3.8, standard error [SE] 0.1), appropriate (mean 3.8, SE 0.1), and feasible (mean 3.9, SE 0.1) on a 5-point Likert scale of agreeability. Perceived barriers to uptake included challenges in patient identification, potential for drug toxicity underreporting, and reimbursement concerns. The authors conclude that the results of this pilot randomized controlled trial of a text message-based e-triage supports further investigation into the use of text message-based symptom reporting by patients as a strategy to safely assess readiness for treatment and thus reduce the time toxicity associated with cancer care.
Figures




References
-
- Bange EM, Doucette A, Gabriel PE, et al. Opportunity costs of receiving palliative chemotherapy for metastatic pancreatic ductal adenocarcinoma. JCO Oncol Pract 2020;16:e678–e687. https://pmc.ncbi.nlm.nih.gov/articles/PMC7427417/. 10.1200/JOP.19.00328 - DOI - PMC - PubMed
-
- Gupta A, Eisenhauer EA, Booth CM. The time toxicity of cancer treatment. J Clin Oncol 2022;40:1611–1615. https://ascopubs.org/doi/10.1200/JCO.21.02810. 10.1200/JCO.21.02810 - DOI - DOI - PubMed
-
- Presley CJ, Soulos PR, Tinetti M, Montori VM, Yu JB, Gross CP. Treatment burden of Medicare beneficiaries with stage I non–small-cell lung cancer. J Oncol Pract 2017;13:e98–e107. https://pmc.ncbi.nlm.nih.gov/articles/PMC5659117/. 10.1200/JOP.2016.014100 - DOI - PMC - PubMed
-
- Prasad V, Olivier T, Chen EY, Haslam A. Estimation of time cost of anti-cancer drugs approved based on comparisons to best supportive care: a cross sectional analysis. J Cancer Policy 2022;34:100363. https://www.sciencedirect.com/science/article/pii/S221353832200042X. 10.1016/j.jcpo.2022.100363 - DOI - PubMed
-
- Rocque GB, Williams CP, Ingram SA, et al. Health care-related time costs in patients with metastatic breast cancer. Cancer Med 2020;9:8423–8431. https://pmc.ncbi.nlm.nih.gov/articles/PMC7666754/. 10.1002/cam4.3461 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources