

Development and implementation of an "Internet " integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals: A randomized controlled trial
- PMID: 40693253
- PMCID: PMC12277550
- DOI: 10.1177/20552076251357657
Development and implementation of an "Internet " integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals: A randomized controlled trial
Abstract
Objective: This study investigates the effects of developing and implementing an integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals under the deep integration of Internet technology. The goal is to provide practical references for addressing declining birth rate challenges and promoting the sustainable development of maternal and child specialty hospitals.
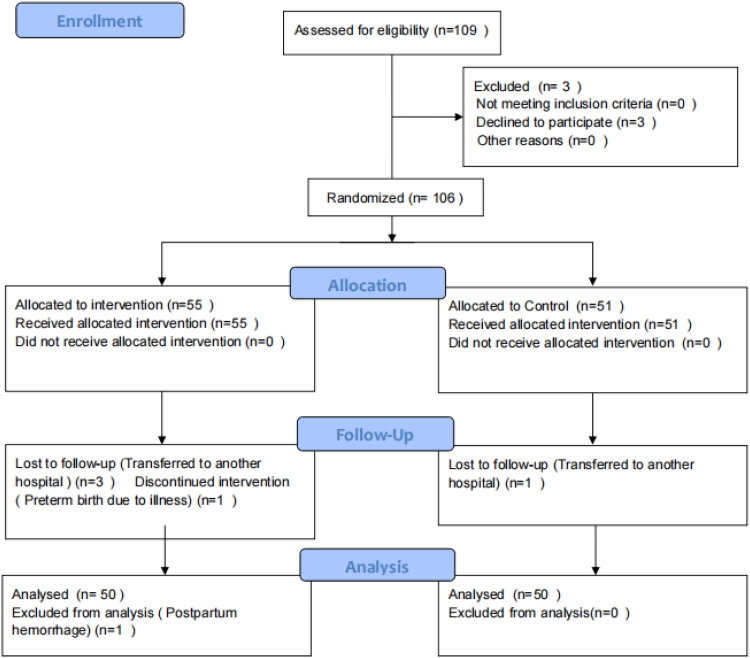
Methods: Using a convenience sampling method, 100 pregnant and postpartum women from a tertiary maternal and child health hospital in Chengdu, China, were selected as the participants for this study. A random number table was used to assign the participants into the control group and the intervention group, with 50 participants in each group. The control group received conventional nursing care, while the intervention group was provided with an integrated service model for antepartum, intrapartum, and postpartum care, fully implemented with Internet technology. A comprehensive comparative analysis was conducted between the two groups across several key dimensions, including the number of return visits within 42 days postpartum: The actual number of return visits for checkups, treatments, or consultations due to various health issues during this period was recorded and compared; Postpartum complications within 42 days: The occurrence rates of common complications, such as postpartum infections, hemorrhage, and milk stasis, were meticulously documented and analyzed for both groups. Service satisfaction: A nursing satisfaction questionnaire was used to objectively and comprehensively assess the satisfaction levels of participants in both groups with the care they received. Willingness for postpartum follow-up visits: Differences in participants' subjective willingness and proactive attitudes toward arranging subsequent postpartum visits were thoroughly examined. Psychological indicators: Using psychological assessment scales, the psychological status of the two groups was evaluated from the establishment of personal health records to postpartum follow-up, analyzing the psychological differences between the two groups.
Results: Through systematic data collection, organization, and rigorous statistical analysis, the results revealed that the average number of return visits within 42 days postpartum was significantly lower in the intervention group (0.16 ± 0.42) compared to the control group (1.44 ± 1.11) (t = -7.630, P < .001). For service satisfaction, 84.00% (42/50) of participants in the intervention group were very satisfied, significantly higher than 52.00% (26/50) in the control group (χ² = 3.170, P = .001). The incidence of mastitis within 42 days postpartum was 2.00% (1/50) in the intervention group, markedly lower than 28.00% (14/50) in the control group (χ² = 2.670, P < .001). For willingness to seek follow-up visit, 96.00% (48/50) of participants in the intervention group stated they would return to the hospital if they had health issues, compared to 82.00% (41/50) in the control group (χ² = 5.010, P = .025). 92.00% (46/50) of participants in the intervention group were willing to choose our hospital for the newborn's health checkup, significantly higher than 76.00% (38/50) in the control group (χ² = 61.060, P < .001). The 28 weeks GAD-7 scored lower in the intervention group (4.14 ± 0.73) than in the control group (5.27 ± 1.00) (t = -6.430, P < .001) and also lower in the intervention group than in the control group at admission (5.58 ± 1.40 vs. 7.29 ± 1.61; t = -5.630, P < .001). There was no significant difference in 28 weeks EPDS scores between two groups (9.02 ± 0.68 vs. 9.18 ± 0.78; t = -1.110, P = .270). The intervention group showed significantly lower EPDS scores at 42 days postpartum (7.84 ± 0.71 vs. 9.61 ± 1.84; t = -6.310, P < .001).
Conclusion: The integrated service model for antepartum, intrapartum, and postpartum care in maternal and child specialty hospitals, based on the "Internet+" concept, effectively integrates Internet technology with critical processes in nursing services. This model precisely and efficiently addresses pregnant and postpartum women's unique maternal and childcare needs at different physiological stages. It demonstrates significant advantages in optimizing medical resource allocation, improving the quality and efficiency of nursing services, and enhancing patients' healthcare experiences and trust. The findings of this empirical study provide robust evidence for the model's effectiveness in nursing care. The successful implementation of this innovative service model offers new perspectives and directions for transforming and upgrading maternal and child specialty hospitals in the face of declining birth rates and the associated challenges and opportunities. It holds significant value for broader application and promotion, with promising prospects for further development.
Keywords: Internet+; antepartum; intrapartum; nursing care; postpartum; service model.
© The Author(s) 2025.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Nutritional interventions for survivors of childhood cancer.Cochrane Database Syst Rev. 2016 Aug 22;2016(8):CD009678. doi: 10.1002/14651858.CD009678.pub2. Cochrane Database Syst Rev. 2016. PMID: 27545902 Free PMC article.
-
Oxytocin for preventing postpartum haemorrhage (PPH) in non-facility birth settings.Cochrane Database Syst Rev. 2016 Apr 14;4(4):CD011491. doi: 10.1002/14651858.CD011491.pub2. Cochrane Database Syst Rev. 2016. PMID: 27078125 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
References
-
- Anger HA, Durocher J, Dabash R, et al. Postpartum infection, pain and experiences with care among women treated for postpartum hemorrhage in three African countries: a cohort study of women managed with and without condom-catheter uterine balloon tamponade[J]. PLoS One 2021; 16: e0245988. - PMC - PubMed
-
- Zhou Y, Yang L, Ling J, et al. Research on the application of nursing intervention of internet + whole course breastfeeding support in cesarean section women [J]. Chin J Nurs 2024; 16: 1933–1941.
LinkOut - more resources
Full Text Sources
