

The Role of Hydroxychloroquine in the Management of Rheumatic Disorders: A Comprehensive Review
- PMID: 40693372
- PMCID: PMC12281268
- DOI: 10.1111/bcpt.70082
The Role of Hydroxychloroquine in the Management of Rheumatic Disorders: A Comprehensive Review
Abstract
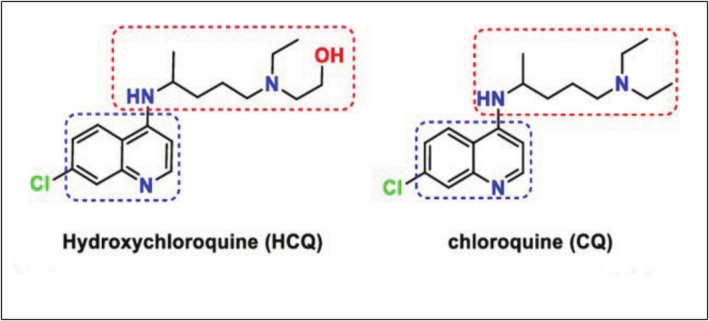
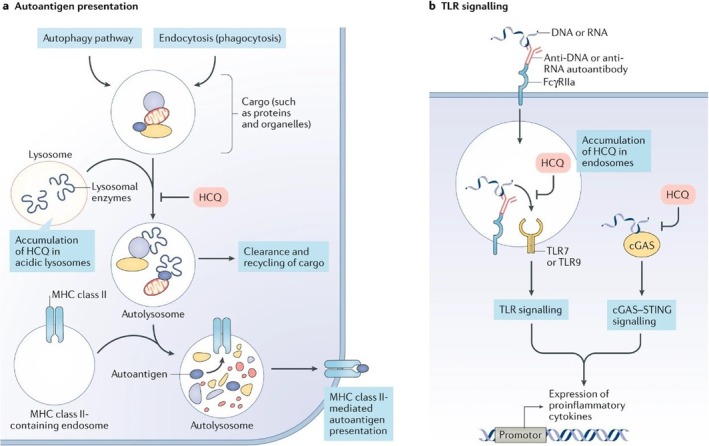
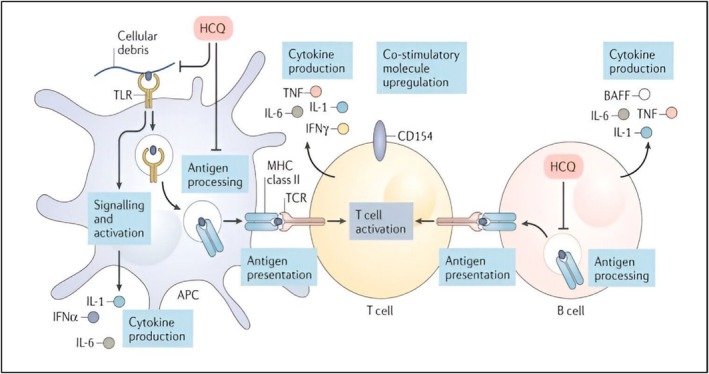
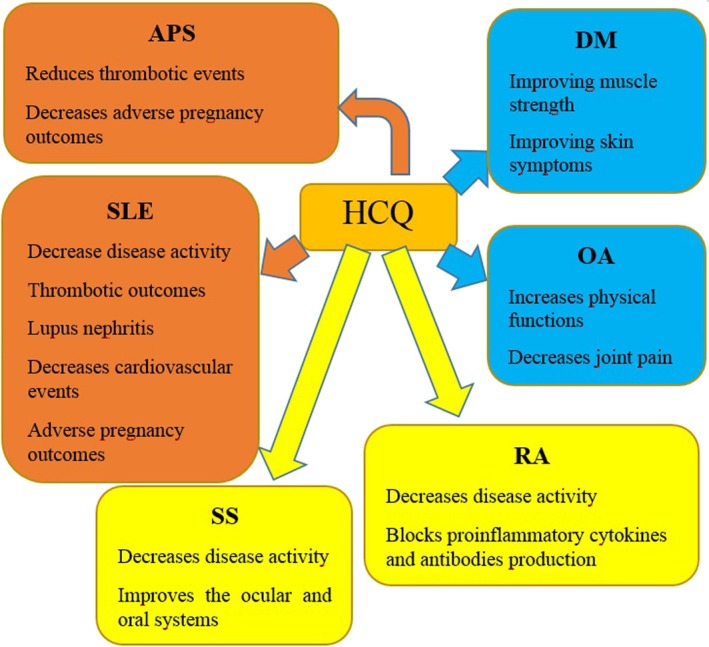
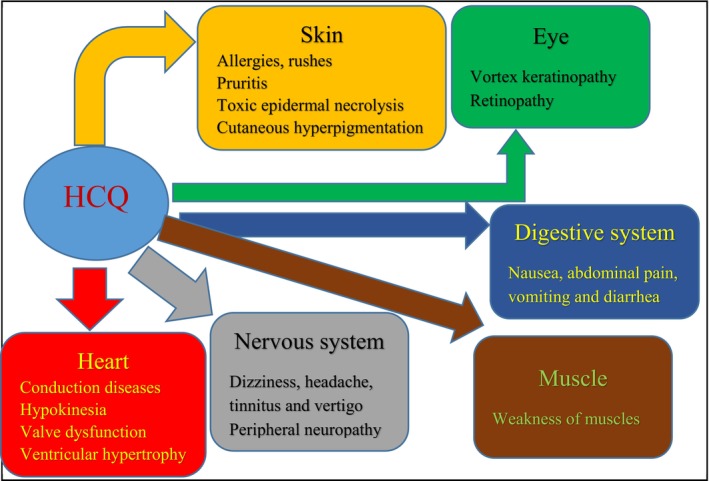
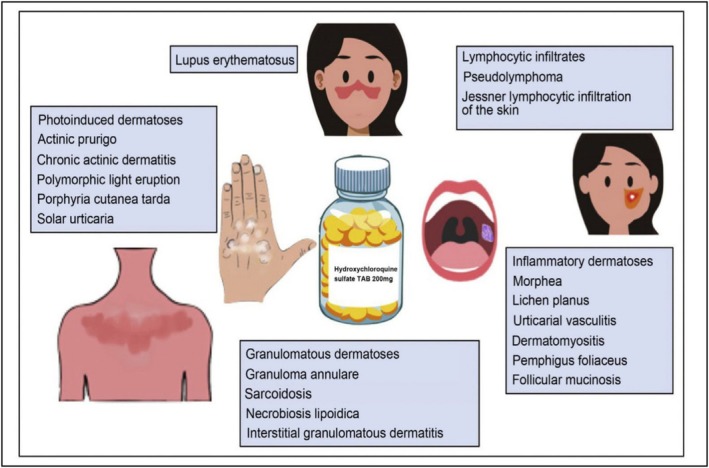
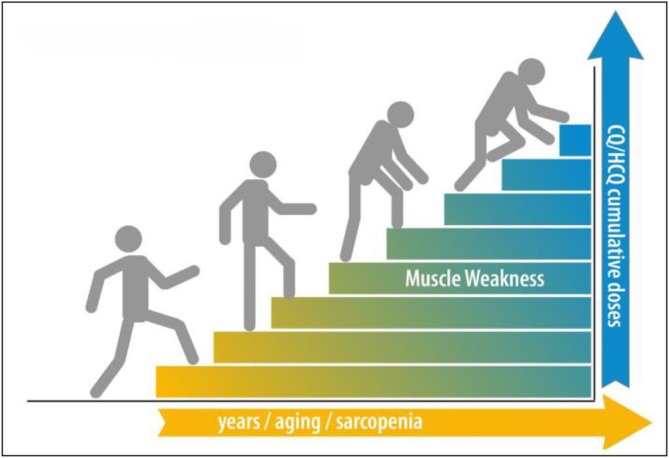
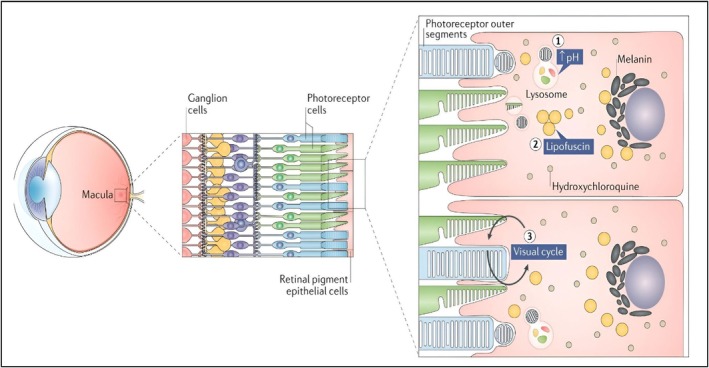
A drug preferred for its antimalarial effect called hydroxychloroquine (HCQ) has long been used to manage and avoid malaria. Nevertheless, its exact mode of action is still unknown. HCQ works through a variety of strategies to influence distinct molecular and cellular pathways. Additionally, HCQ has been demonstrated to be an effective treatment for rheumatic conditions such as primary Sjögren's syndrome, rheumatoid arthritis, antiphospholipid syndrome and systemic lupus erythematosus. Despite being widely regarded as safe, HCQ has been known to cause adverse responses; thus, doctors should closely evaluate rheumatism patients before taking these medications. The current study aims to emphasize the potential side effects of treatment while supporting the clinical usage of HCQ for autoimmune disorders.
Keywords: effect mechanisms; hydroxychloroquine; organ toxicity; rheumatic disorders.
© 2025 The Author(s). Basic & Clinical Pharmacology & Toxicology published by John Wiley & Sons Ltd on behalf of Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Puolakka K., Kautiainen H., Möttönen T., et al., “Impact of Initial Aggressive Drug Treatment With a Combination of Disease‐Modifying Antirheumatic Drugs on the Development of Work Disability in Early Rheumatoid Arthritis: A Five‐Year Randomized Followup Trial,” Arthritis Rheum 50, no. 1 (2004): 55–62, 10.1002/art.11436. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
