

Multizonal outer retinopathy and retinal pigment epitheliopathy (MORR) with a chronologically divergent presentation- a case report
- PMID: 40694285
- PMCID: PMC12283491
- DOI: 10.1186/s12348-025-00519-0
Multizonal outer retinopathy and retinal pigment epitheliopathy (MORR) with a chronologically divergent presentation- a case report
Abstract
Purpose: Acute zonal occult outer retinopathy (AZOOR) is a rare inflammatory disease of the outer retina, often presented with subtle early findings. A specific subtype, termed Multizonal Outer Retinopathy and Retinal Pigment Epitheliopathy (MORR), is characterized by distinct progression pattern (Ramtohul et al. Retina 43:1890–1903, 2023) in multiple zones of the outer retina and retinal pigment epithelium. This case report aims to illustrate the chronologically divergent presentation, a phase-shifting disease progression and the complex clinical course of MORR, and to discuss the diagnostic challenges posed by its phase‑shifted timeline as well as potential therapeutic options.
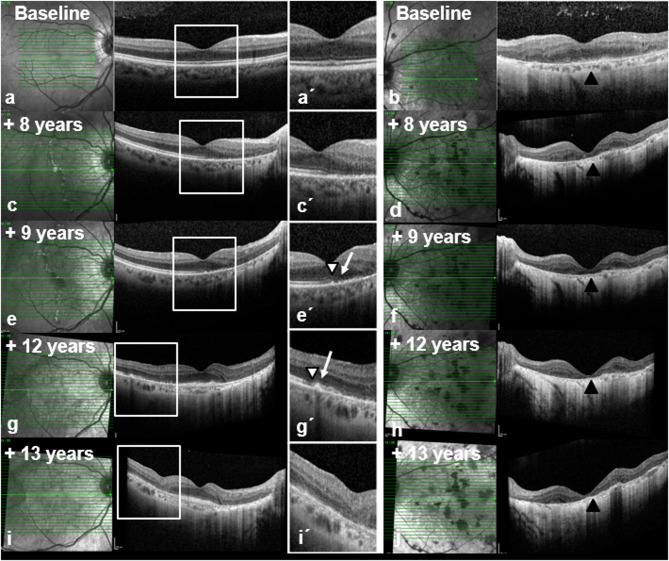
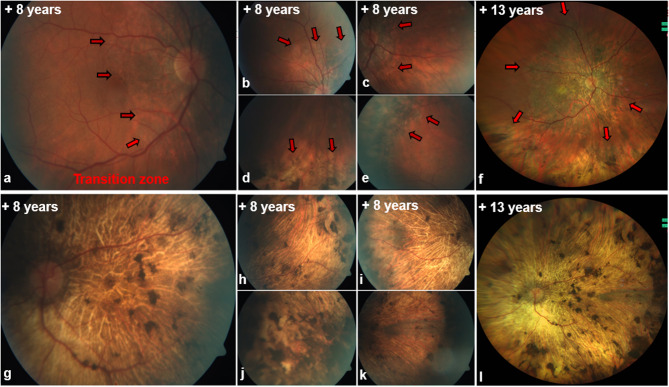
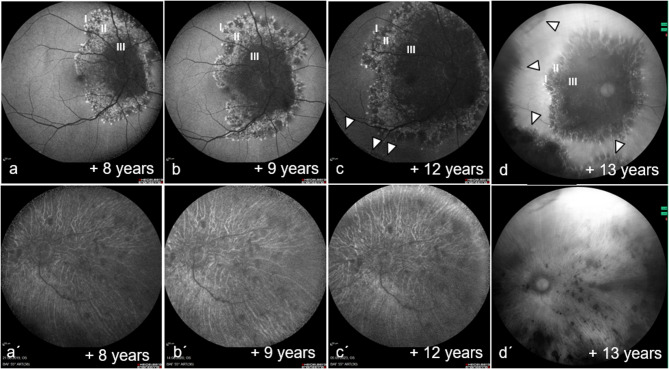
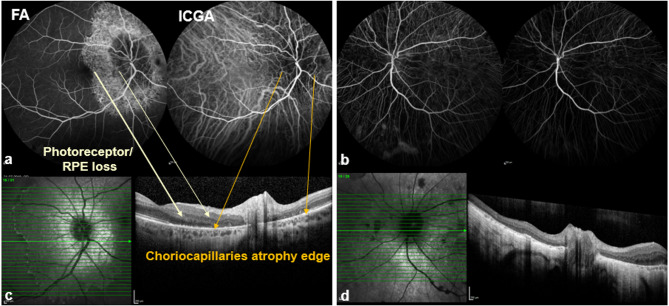
Methods: A case of a 52-year-old female patient with initially unilateral, inactive posterior uveitis was retrospectively analyzed. Over thirteen years, progressive functional impairment developed in the fellow eye. Findings were assessed using multimodal imaging (Optical Coherence Tomography [OCT], Fundus Autofluorescence [FAF], Fluorescein and Indocyanine Green Angiography [FFA/ICGA]) and electrophysiological examinations (multifocal ERG, full-field ERG, EOG, VEP). Additional rheumatologic and neurologic assessments were conducted, and an infectious workup was performed.
Results: The patient demonstrated chronologically divergent bilateral involvement with extensive damage to the retinal pigment epithelium (RPE) and photoreceptors. Fundus autofluorescence revealed a tri- to multizonal pattern in the better eye, while the fellow eye already exhibited diffuse atrophic areas devoid of any autofluorescence. Electrophysiological, the better eye showed selectively prolonged latencies on multifocal electroretinography (multifocal ERG) but preserved amplitudes, whereas the more severely affected eye displayed substantial functional loss. Despite various therapeutic interventions, including high-dose corticosteroids and immunosuppressive agents, progressive visual impairment ensued, driven by increasing macular involvement.
Conclusions: This case highlights the marked heterogeneity and diagnostic complexities of Multizonal Outer Retinopathy and Retinal Pigment Epitheliopathy (MORR), a newly recognized progressive variant of Acute Zonal Occult Outer Retinopathy (AZOOR). The disease course can present with chronologically divergent manifestations in both eyes. While initial stages may exhibit only subtle funduscopic changes, structural and functional deficits can progress rapidly, episodically and in a phase-shifted manner. Multimodal imaging is essential to delineate the disease trajectory and to distinguish MORR from diseases affecting outer retina. Currently, no definitive treatment is available; although immunomodulatory therapies may stabilize the condition in certain cases, their efficacy remains inconsistent. Consequently, early low-vision management and close interdisciplinary collaboration are of particular importance.
Keywords: Acute zonal occult outer retinopathy; Course; Multimodal imaging; Multizonal outer retinopathy and retinal pigment epitheliopathy.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The authors declare no conflict of interest. No studies on humans or animals were conducted by the authors for this paper. For the studies listed, the ethical guidelines stated therein apply in each case. Consent for publication: Written consent has been obtained from patients and/or their legal representatives for images or other information within the manuscript that can be used to identify patients. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
A case documenting distinct natural history of multizonal outer retinopathy and retinal pigment epitheliopathy (MORR) with longitudinal multi-modal documentation of progression.Am J Ophthalmol Case Rep. 2024 Nov 29;36:102222. doi: 10.1016/j.ajoc.2024.102222. eCollection 2024 Dec. Am J Ophthalmol Case Rep. 2024. PMID: 39697673 Free PMC article.
-
MULTIZONAL OUTER RETINOPATHY AND RETINAL PIGMENT EPITHELIOPATHY (MORR): A Newly Recognized Entity or an Unusual Variant of AZOOR?Retina. 2023 Nov 1;43(11):1890-1903. doi: 10.1097/IAE.0000000000003927. Epub 2023 Oct 19. Retina. 2023. PMID: 37748093 Free PMC article.
-
Current understanding of acute zonal occult outer retinopathy (AZOOR).Indian J Ophthalmol. 2024 Jul 1;72(7):935-937. doi: 10.4103/IJO.IJO_3228_23. Epub 2024 Mar 8. Indian J Ophthalmol. 2024. PMID: 38454854 Free PMC article. Review.
-
Clinical course of acute zonal occult outer retinopathy complicated by choroidal neovascularization.Int J Retina Vitreous. 2018 Aug 29;4:32. doi: 10.1186/s40942-018-0134-y. eCollection 2018. Int J Retina Vitreous. 2018. PMID: 30181904 Free PMC article.
-
Application of Ophthalmic Electrophysiology in Inflammatory Disorders of Retina and Optic Nerve.J Clin Med. 2024 Jun 29;13(13):3829. doi: 10.3390/jcm13133829. J Clin Med. 2024. PMID: 38999396 Free PMC article. Review.
References
-
- Gass JD (1993) Acute zonal occult outer retinopathy. Donders lecture: the Netherlands ophthalmological society, maastricht, holland, June 19, 1992. J Clin Neuroophthalmol 13(2):79–97 - PubMed
-
- Félix-Espinar B, Moreno-López M (2021) Use of multimodal analysis in the diagnosis and Follow-up of a case of acute zonal occult outer retinopathy (AZOOR). Arch Soc Esp Oftalmol (Engl Ed) 96(12):658–662 - PubMed
-
- Pohlmann D, Winterhalter S, Pleyer U (2019) White Dot syndromes: principles, diagnostics, and treatment. Ophthalmologe 116(12):1235–1256 - PubMed
-
- Monson DM, Smith JR (2011) Acute zonal occult outer retinopathy. Surv Ophthalmol 56(1):23–35 - PubMed
LinkOut - more resources
Full Text Sources
