

Application of flexible parametric cure model in determination of effective factors on the technique of survival peritoneal dialysis patients in adults of Iran
- PMID: 40694578
- PMCID: PMC12282859
- DOI: 10.1371/journal.pone.0326748
Application of flexible parametric cure model in determination of effective factors on the technique of survival peritoneal dialysis patients in adults of Iran
Abstract
Objective: Peritoneal Dialysis (PD) is one of the most common methods of dialysis performed in patients with kidney failure. This study presents the application of flexible parametric cure models, which enhance fit and interpretability by accommodating various survival distributions and allowing for the estimation of the cured fraction in diverse populations. Thus, the purpose of this study is to determine the risk and demographic factors affecting the survival of non-cured dialysis patients undergoing peritoneal dialysis, as well as to estimate the cured fraction of survival using this method.
Methodology: A total of 4,144 adult patients (aged 20 and above) were included in a retrospective (historical) cohort study from the Iranian PD registry, conducted between 1995 and 2018 across 20 centers nationwide. The study considered important variables such as sex, age, BMI, creatinine, calcium, cholesterol, triglycerides, Low-Density Lipoprotein (LDL), High-Density Lipoprotein (HDL), Erythrocyte Sedimentation Rate (ESR), systolic blood pressure (SBP), and diastolic blood pressure (DBP). A flexible parametric cure model was employed to assess the independent risk factors for PD technique failure.
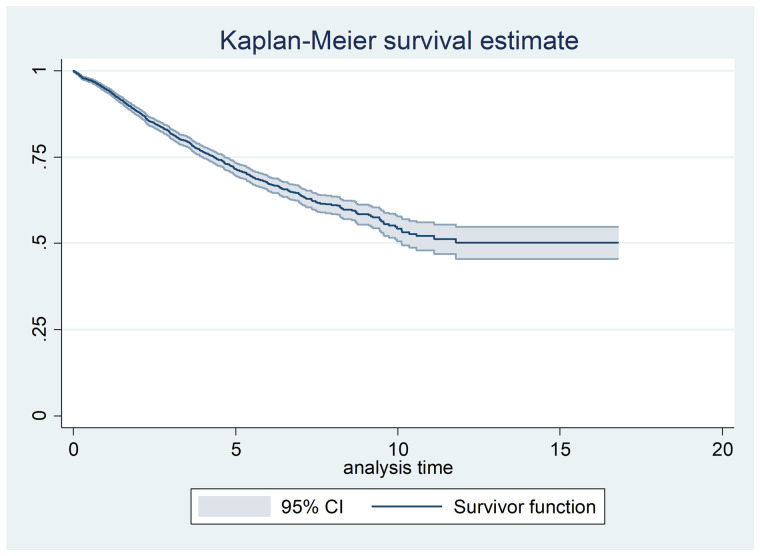
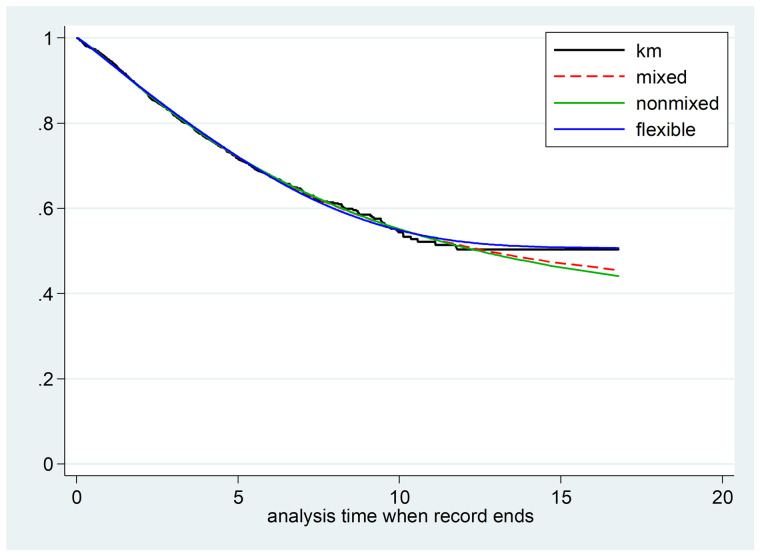
Findings: The results of the current study showed that the flexible parametric cure Model (AIC = 5735.06) has a better fit compared with another cure model (mixture cure model = 6676.25, non-mixture cure model = 6677.28). Based on the findings of this study, the estimated cure fraction of survival using the PD method was 50% (95% CI: 0.47-0.53). The flexible cure model, demonstrated in a multivariate setting, indicated that variables such as age over 60 years (HR = 2.11, 95% CI: 1.05-1.35), calcium levels above 10.2 (HR = 1.43, 95% CI: 1.30-1.56), LDL levels above 140 (HR = 1.23 95% CI: 1.07-1.42), ESR (HR = 1.006, 95% CI: 1.003-1.01) and DBP (HR = 1.17, 95% CI: 1.16-1.31) significantly impacted the survival of non-cured patients.
Conclusion: The presence of cured individuals in the data flattens the Kaplan-Meier curve. In such cases, employing a flexible parametric cure model is appropriate to separately investigate the effects of various factors on the cure fraction and the survival of susceptible individuals. The findings of this study indicated that age, calcium, LDL, ESR, and DBP significantly influenced the survival of non-cured individuals. Specifically, increases in these variables were associated with a higher risk of technique failure.
Copyright: © 2025 Karimi Ghahfarokhi et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Sex and gender as predictors for allograft and patient-relevant outcomes after kidney transplantation.Cochrane Database Syst Rev. 2024 Dec 19;12(12):CD014966. doi: 10.1002/14651858.CD014966.pub2. Cochrane Database Syst Rev. 2024. PMID: 39698949
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Automated peritoneal dialysis versus continuous ambulatory peritoneal dialysis for people with kidney failure.Cochrane Database Syst Rev. 2024 Sep 11;9(9):CD006515. doi: 10.1002/14651858.CD006515.pub2. Cochrane Database Syst Rev. 2024. PMID: 39258519
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
References
-
- Krishnan M, Thodis E, Ikonomopoulos D, Vidgen E, Chu M, Bargman JM, et al. Predictors of outcome following bacterial peritonitis in peritoneal dialysis. Perit Dial Int. 2002;22(5):573–81. - PubMed
-
- Mojdeh S, Karimi S, Mehrabi A, Bakhtiari S. Etiology of renal failure and peritoneal dialysis complications in Isfahan. Health. 2013;2013.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
