

TME-guided deep learning predicts chemotherapy and immunotherapy response in gastric cancer with attention-enhanced residual Swin Transformer
- PMID: 40695288
- PMCID: PMC12432364
- DOI: 10.1016/j.xcrm.2025.102242
TME-guided deep learning predicts chemotherapy and immunotherapy response in gastric cancer with attention-enhanced residual Swin Transformer
Abstract
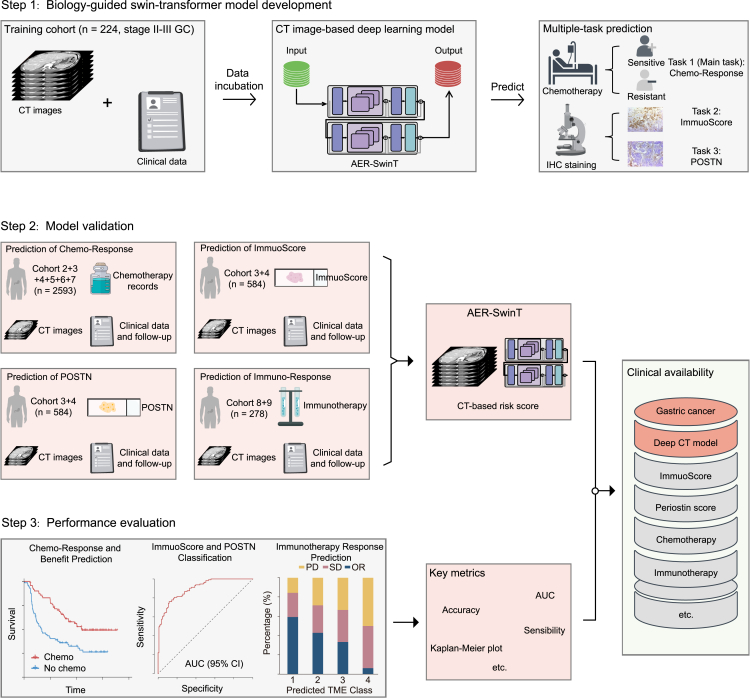
Adjuvant chemotherapy and immune checkpoint blockade exert quite durable anti-tumor responses, but the lack of effective biomarkers limits the therapeutic benefits. Utilizing multi-cohorts of 3,095 patients with gastric cancer, we propose an attention-enhanced residual Swin Transformer network to predict chemotherapy response (main task), and two predicting subtasks (ImmunoScore and periostin [POSTN]) are used as intermediate tasks to improve the model's performance. Furthermore, we assess whether the model can identify which patients would benefit from immunotherapy. The deep learning model achieves high accuracy in predicting chemotherapy response and the tumor microenvironment (ImmunoScore and POSTN). We further find that the model can identify which patient may benefit from checkpoint blockade immunotherapy. This approach offers precise chemotherapy and immunotherapy response predictions, opening avenues for personalized treatment options. Prospective studies are warranted to validate its clinical utility.
Keywords: chemotherapy response; immunotherapy; medical imaging; multitask Swin Transformer; tumor microenvironment.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures




References
-
- Zhang X., Liang H., Li Z., Xue Y., Wang Y., Zhou Z., Yu J., Bu Z., Chen L., Du Y., et al. Perioperative or postoperative adjuvant oxaliplatin with S-1 versus adjuvant oxaliplatin with capecitabine in patients with locally advanced gastric or gastro-oesophageal junction adenocarcinoma undergoing D2 gastrectomy (RESOLVE): an open-label, superiority and non-inferiority, phase 3 randomised controlled trial. Lancet Oncol. 2021;22:1081–1092. doi: 10.1016/S1470-2045(21)00297-7. - DOI - PubMed
-
- Noh S.H., Park S.R., Yang H.K., Chung H.C., Chung I.J., Kim S.W., Kim H.H., Choi J.H., Kim H.K., Yu W., et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15:1389–1396. doi: 10.1016/S1470-2045(14)70473-5. - DOI - PubMed
-
- Sundar R., Tan P. Genomic Analyses and Precision Oncology in Gastroesophageal Cancer: Forwards or Backwards? Cancer Discov. 2018;8:14–16. doi: 10.1158/2159-8290.CD-17-1295. - DOI - PubMed
-
- Janjigian Y.Y., Ajani J.A., Moehler M., Shen L., Garrido M., Gallardo C., Wyrwicz L., Yamaguchi K., Cleary J.M., Elimova E., et al. First-Line Nivolumab Plus Chemotherapy for Advanced Gastric, Gastroesophageal Junction, and Esophageal Adenocarcinoma: 3-Year Follow-Up of the Phase III CheckMate 649 Trial. J. Clin. Oncol. 2024;42:2012–2020. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
