

Liberation from invasive mechanical ventilation: a nationwide survey among intensive care units in the Netherlands
- PMID: 40695529
- PMCID: PMC12281335
- DOI: 10.1136/bmjresp-2024-002868
Liberation from invasive mechanical ventilation: a nationwide survey among intensive care units in the Netherlands
Abstract
Background: Liberation from invasive mechanical ventilation is a milestone in critical care, but approaches vary. This survey aimed to describe current ventilator liberation practices, relate them to available evidence, and identify areas for improvement.
Methods: A survey was performed among Dutch intensive care unit (ICU) sites. The survey evaluated practice in seven domains of ventilator liberation: protocol availability, transition from controlled to assisted ventilation, spontaneous breathing trials (SBT), cuff-leak test, postextubation support, weaning failure and tracheostomised weaning.
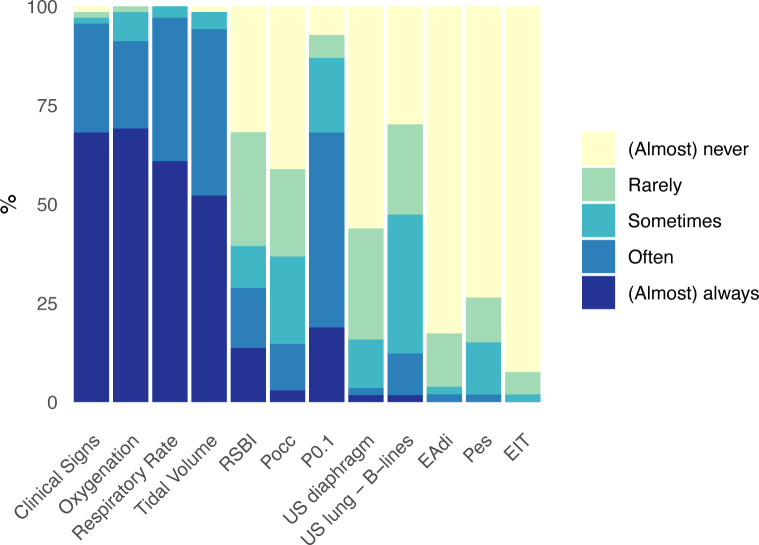
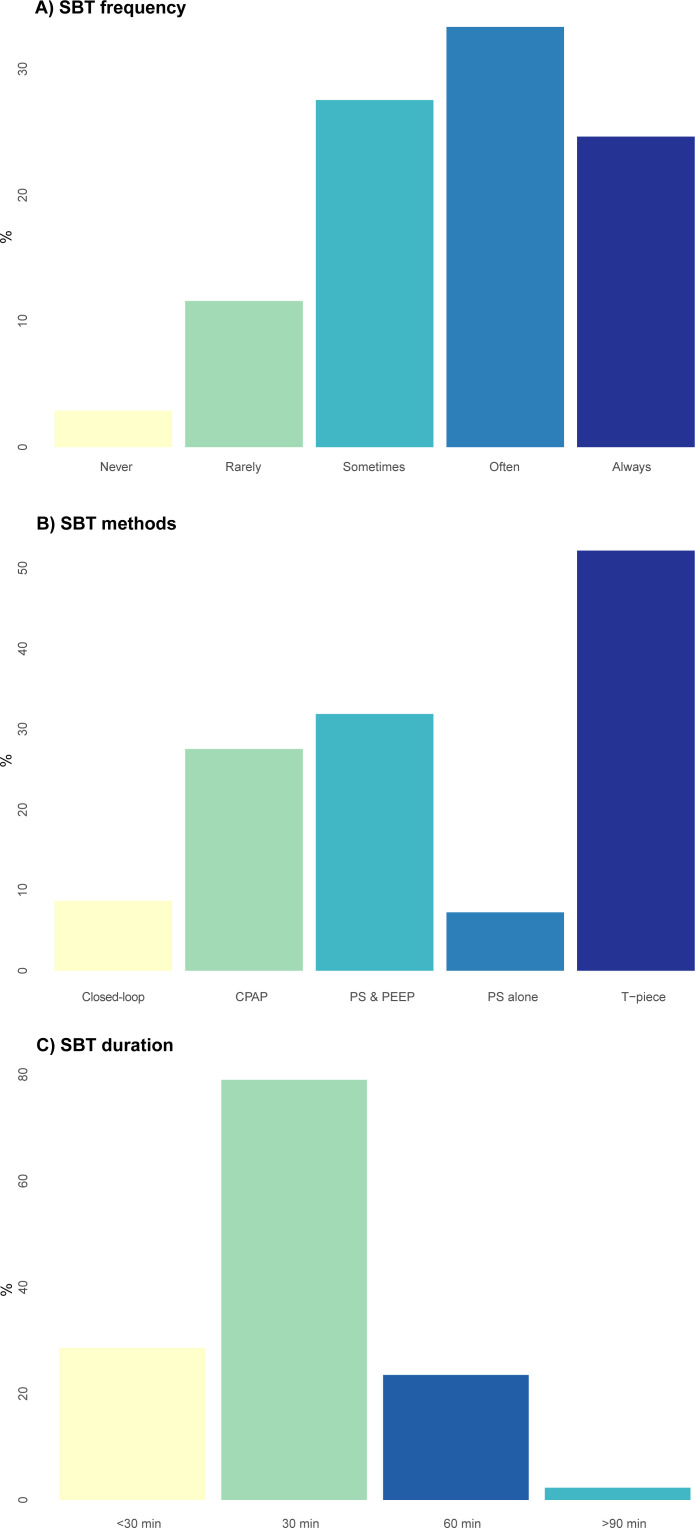
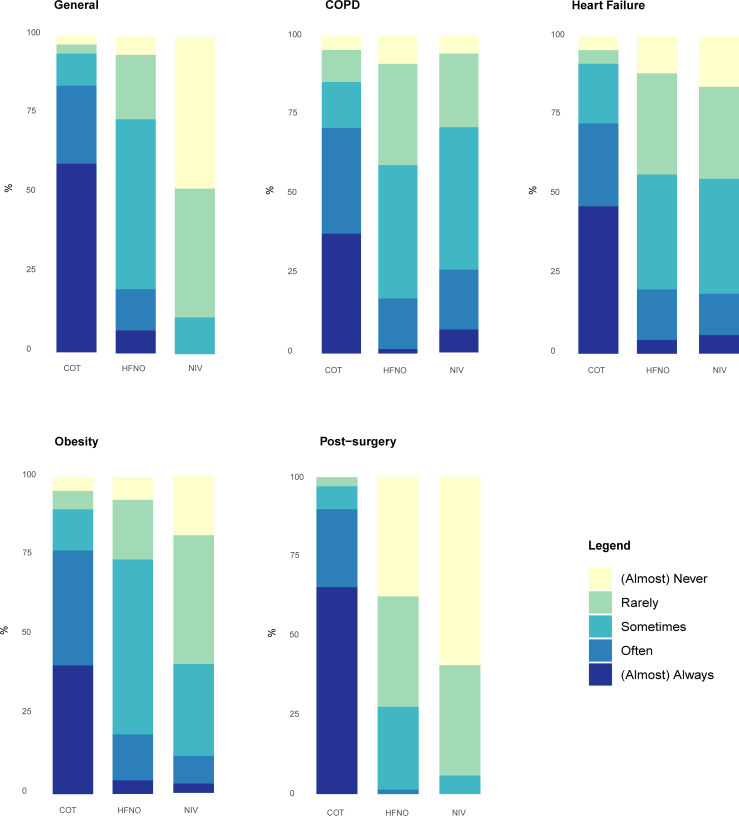
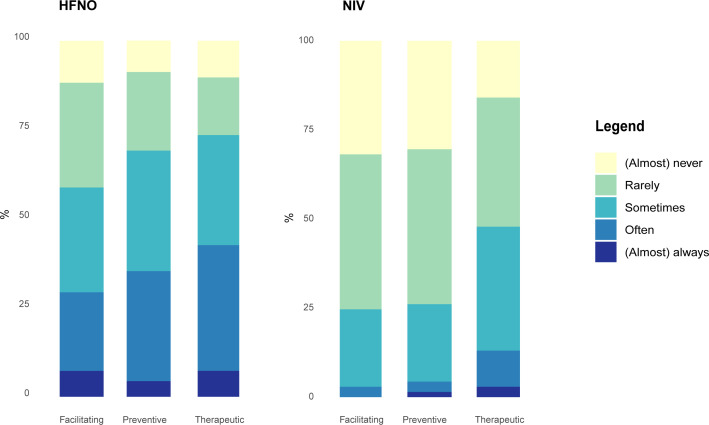
Results: The survey response rate was 93% (132/142), representing 97% (69/71) of Dutch ICUs. Protocols for postextubation support and weaning failure were available in less than half of the ICUs (44% and 49%, respectively). The transition from controlled to assisted ventilation is regularly evaluated daily in 78% of ICUs. Assisted ventilation tolerance is mainly assessed by clinical signs, respiratory parameters and non-invasive manoeuvres that assess respiratory drive (P0.1). SBTs are regularly performed in 58% of ICUs, using one or more of the following methods: T-piece (52%), pressure support+positive end expiratory pressure (32%) and continuous positive airway pressure (28%). Cuff-leak tests are seldom performed (1.4%), predominantly in cases of intubation for upper-airway obstruction (92%). Postextubation respiratory support with high-flow nasal oxygen or non-invasive ventilation is used at least as often with therapeutic (43%/13%) rather than preventive (35%/4%) of facilitative intent (29%/3%). Delirium screening (87%) and reconsidering sedation (84%) are frequently assessed in case of weaning failure. Regular use of closed-loop ventilation is reported in a minority of ICUs throughout the process of ventilator liberation (3-9%).
Conclusions: Various aspects of ventilator liberation practices show only limited alignment with existing guidelines. The results of this survey pinpoint areas to prioritise in guideline and practice improvement.
Keywords: Critical Care; Surveys and Questionnaires.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: HE has received unrestricted research grants from ZonMW (Netherlands), Fisher & Paykel Healthcare (Auckland, New Zealand), Roche Diagnostics Ltd. (Basel, Switzerland) and Ventinova Medical B.V. (Eindhoven, the Netherlands), and speakers fee from Getinge (Sweden). LMAH has received speakers fee from Getinge (Sweden), research support from Liberate Medical (Crestwood, Kentucky), ZonMw (Netherlands) and the European Respiratory Society, and personal fees from American Thoracic Society. Other authors: no interests to declare.
Figures
References
-
- Provost KA, El-Solh AA. New York, NY: McGraw-Hill Education; 2012. Complications associated with mechanical ventilation.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical