

Influence of body position and time of day on ocular rhythms
- PMID: 40695902
- PMCID: PMC12284202
- DOI: 10.1038/s41598-025-10873-7
Influence of body position and time of day on ocular rhythms
Abstract
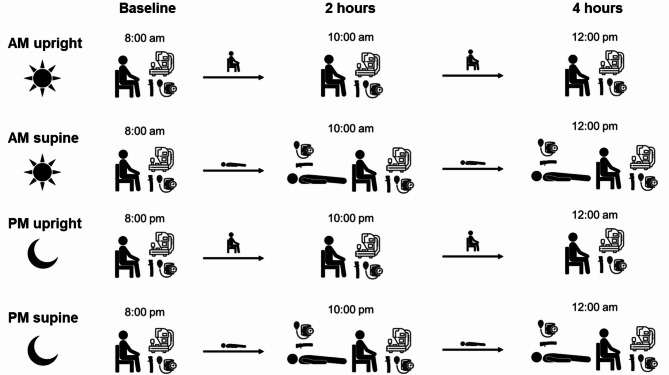
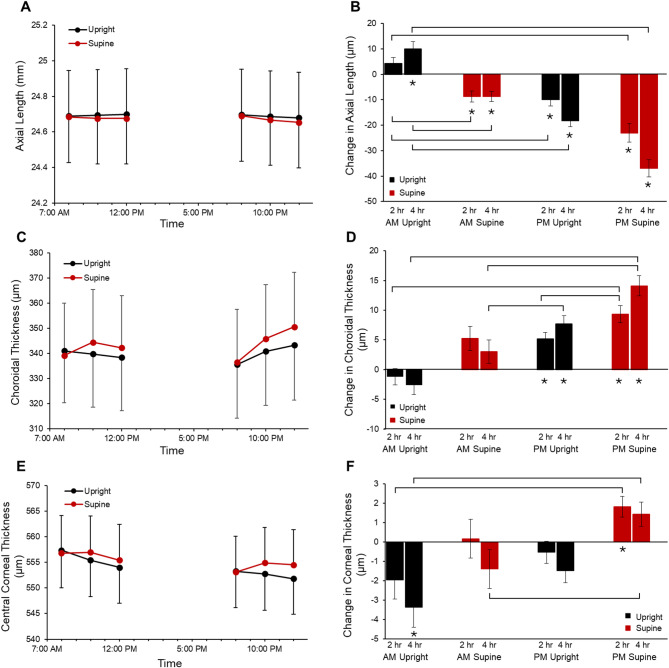
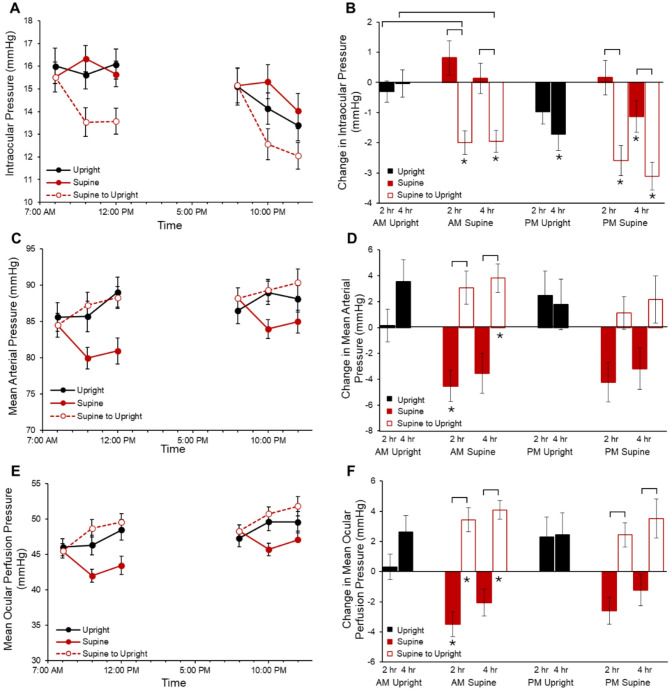
To determine the influence of time of day and body position on axial length, microvasculature, and intraocular pressure (IOP), participants (N = 23, ages 22-46 years) were enrolled in four 4-hour experimental sessions, which varied by time of day (morning or night) and body position (upright or supine). Blood pressure, heart rate, IOP, biometry, and optical coherence tomography (OCT) and OCT angiography (OCTA) imaging were performed every 2 h. For supine sessions, IOP was also measured 10 min after position changed to upright. When upright for 4 h in the morning, axial length increased 10.0 ± 2.8 μm (P = 0.005). When supine in the morning, axial length decreased 8.7 ± 2.2 μm (P < 0.001). When upright at night, axial length decreased 18.3 ± 2.3 μm (P < 0.001), and choroidal thickness increased 7.7 ± 1.4 μm (P < 0.001). When supine at night, axial length decreased 37.0 ± 3.4 μm (P < 0.001) and choroidal thickness increased 14.1 ± 1.7 μm (P < 0.001). IOP measured 10 min after transitioning to an upright position showed an acute decrease (P < 0.05). No significant changes in retinal microvasculature were observed with body position or time (P > 0.05 for all). In conclusion, body position and time of day influence axial length, choroidal thickness, and IOP, indicating that extrinsic factors work in conjunction with diurnal factors to mediate ocular rhythms.
Keywords: Choroid; Circadian rhythm; Intraocular pressure; Posture.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Disclosures: AR: none; LO: Meta, LLC (financial support), Topcon (financial support), Zeiss (consulting).
Figures
References
-
- Holden, B. A. et al. Global prevalence of myopia and high myopia and Temporal trends from 2000 through 2050. Ophthalmology123, 1036–1042 (2016). - PubMed
-
- Jung, S. K., Lee, J. H., Kakizaki, H. & Jee, D. Prevalence of myopia and its association with body stature and educational level in 19-year-old male conscripts in seoul, South Korea. Invest. Ophthalmol. Vis. Sci.53, 5579–5583 (2012). - PubMed
-
- Flitcroft, D. I. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res.31, 622–660 (2012). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
