

Nomogram for predicting mortality in hospitalized patients with infective endocarditis
- PMID: 40695963
- PMCID: PMC12284201
- DOI: 10.1038/s41598-025-12043-1
Nomogram for predicting mortality in hospitalized patients with infective endocarditis
Abstract
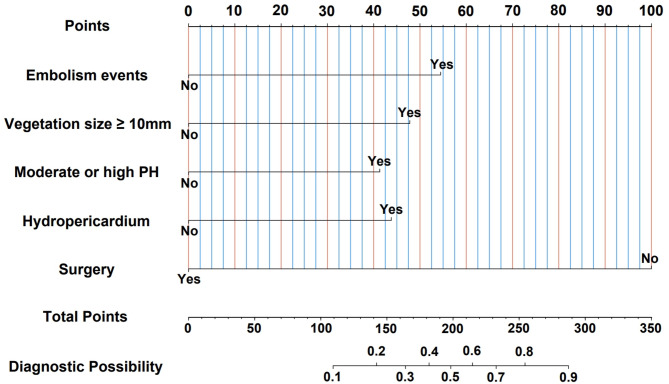
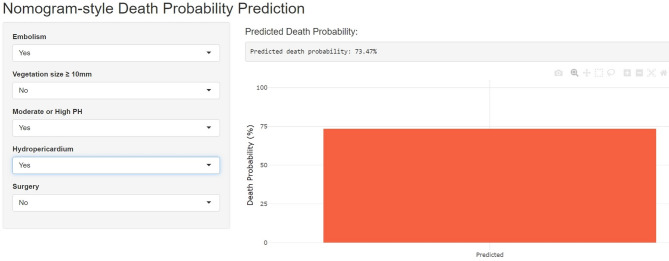
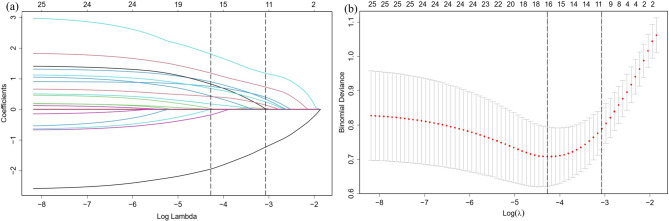
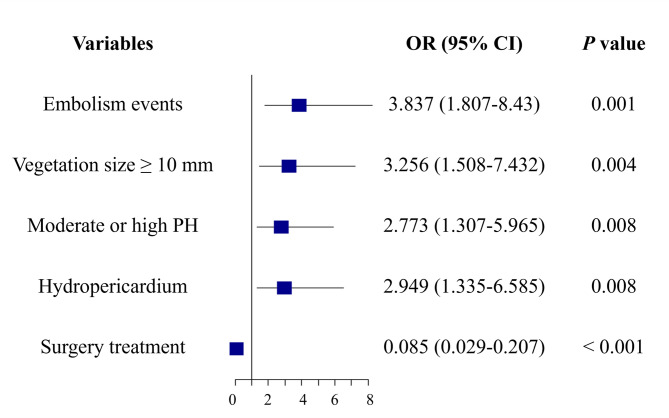
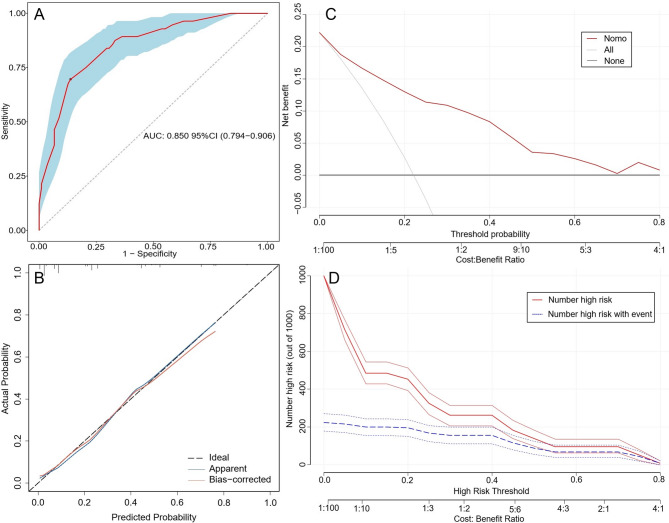
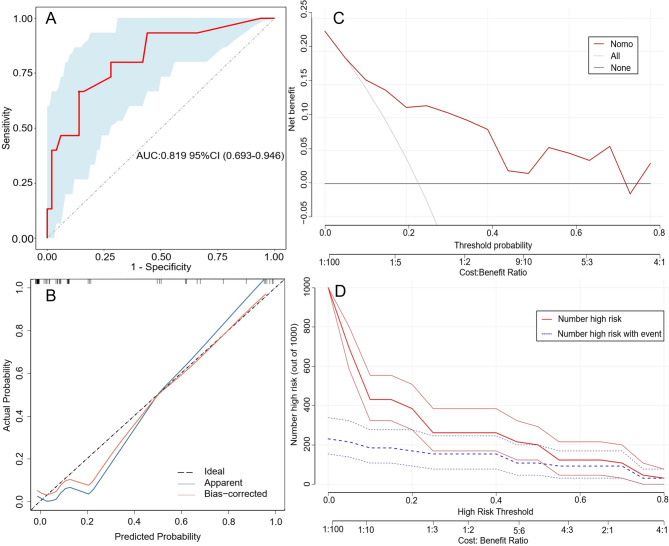
This study aimed to develop a nomogram for accurately predicting in-hospital mortality in patients with infective endocarditis (IE). We conducted a retrospective analysis of clinical, echocardiographic, and laboratory data from IE patients admitted between January 2010 and September 2024. 252 IE patients from the Second Hospital of Lanzhou University were included in the training cohort, while 65 IE patients from the First Hospital of Lanzhou University were enrolled for external validation. The least absolute shrinkage and selection operator (LASSO) regression method was used to identify factors associated with in-hospital mortality. A nomogram was constructed using multivariate logistic regression. Model performance was assessed using receiver operating characteristic (ROC) curve and calibration curve. Clinical utility was evaluated through decision curve analysis (DCA) and clinical impact curve (CIC). The nomogram included five independent risk factors: embolic events, vegetation size ≥ 10 mm, moderate or higher pulmonary hypertension, hydropericardium, and surgery. The area under the curve (AUC) of the nomogram in the training cohort was 0.850 (95% CI: 0.794-0.906), and external validation cohort was 0.819 (95% CI: 0.693-0.946). The calibration plot demonstrated excellent prediction consistency. Both DCA and CIC confirmed the clinical utility of the nomogram. We developed and validated a nomogram for predicting in-hospital mortality in patients with IE. The model demonstrated excellent performance and provided a useful tool to assist clinicians in decision-making and patient management.
Keywords: Infective endocarditis; Mortality; Nomogram; Prediction model.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Development and validation of a nomogram model for predicting the occurrence of necrotizing enterocolitis in premature infants with late-onset sepsis.Eur J Med Res. 2025 Jul 8;30(1):595. doi: 10.1186/s40001-025-02857-0. Eur J Med Res. 2025. PMID: 40629472 Free PMC article.
-
DEVELOPMENT AND VALIDATION OF A NOMOGRAM FOR PREDICTING 28-DAY IN-HOSPITAL MORTALITY IN SEPSIS PATIENTS BASED ON AN OPTIMIZED ACUTE PHYSIOLOGY AND CHRONIC HEALTH EVALUATION II SCORE.Shock. 2024 May 1;61(5):718-727. doi: 10.1097/SHK.0000000000002335. Epub 2024 Feb 5. Shock. 2024. PMID: 38517232
-
A novel nomogram for predicting osteoporosis with low back pain among the patients in Wenshan Zhuang and Miao Autonomous Prefecture of China.Front Endocrinol (Lausanne). 2025 Jun 5;16:1535163. doi: 10.3389/fendo.2025.1535163. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40538801 Free PMC article.
-
Development and Validation of a Nomogram-Based Model to Predict Primary Hypertension Within the Next Year in Children and Adolescents: Retrospective Cohort Study.J Med Internet Res. 2024 Dec 30;26:e58686. doi: 10.2196/58686. J Med Internet Res. 2024. PMID: 39753226 Free PMC article.
-
Radiomics Nomogram Based on Optimal Volume of Interest Derived from High-Resolution CT for Preoperative Prediction of IASLC Grading in Clinical IA Lung Adenocarcinomas: A Multi-Center, Large-Population Study.Technol Cancer Res Treat. 2024 Jan-Dec;23:15330338241300734. doi: 10.1177/15330338241300734. Technol Cancer Res Treat. 2024. PMID: 39569528 Free PMC article.
References
-
- Delgado, V. et al. 2023 ESC guidelines for the management of endocarditis. Eur. Heart J.44, 3948–4042. 10.1093/eurheartj/ehad193 (2023). - PubMed
-
- Li, M., Kim, J. B., Sastry, B. K. S. & Chen, M. Infective endocarditis. Lancet404, 377–392. 10.1016/S0140-6736(24)01098-5 (2024). - PubMed
-
- Hammond-Haley, M. et al. Trends in the incidence and mortality of infective endocarditis in high-income countries between 1990 and 2019. Int. J. Cardiol.371, 441–451. 10.1016/j.ijcard.2022.09.061 (2023). - PubMed
-
- Wilson, W. et al. Prevention of infective endocarditis: Guidelines from the American Heart Association: A guideline from the American Heart Association rheumatic fever, endocarditis, and Kawasaki disease committee, Council on cardiovascular disease in the young, and the Council on clinical cardiology, Council on cardiovascular surgery and anesthesia, and the quality of care and outcomes research interdisciplinary working group. Circulation116, 1736–1754. 10.1161/CIRCULATIONAHA.106.183095 (2007). - PubMed
MeSH terms
Grants and funding
- No. 25ZYJA017/the Central government guides local science and technology development fund projects
- No. 25ZYJA017/the Central government guides local science and technology development fund projects
- No. 25ZYJA017/the Central government guides local science and technology development fund projects
- No. 25ZYJA017/the Central government guides local science and technology development fund projects
- No. 25ZYJA017/the Central government guides local science and technology development fund projects
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
