

Pulmonary arterial hypertension with cardiopulmonary comorbidities: is it a unique phenotype?
- PMID: 40696311
- PMCID: PMC12285108
- DOI: 10.1186/s12890-025-03833-4
Pulmonary arterial hypertension with cardiopulmonary comorbidities: is it a unique phenotype?
Abstract
Background: Pulmonary arterial hypertension (PAH) patients with cardiopulmonary comorbidities have been prevalent nowadays. However, there was limited data on clinical characteristics and therapeutic responses in these populations.
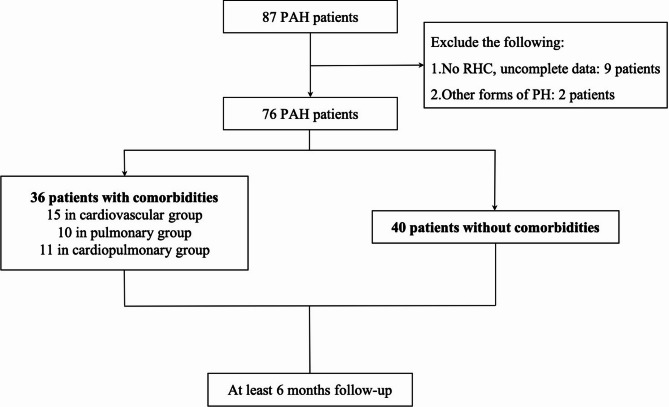
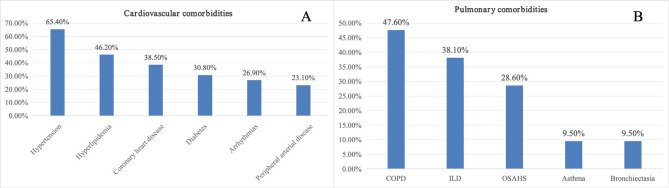
Methods: Patients diagnosed with right heart catheterization (RHC)-confirmed PAH between October 2021 to March 2023 were included in our study. According to whether they had cardiopulmonary diseases or not, they were classified into two groups: comorbidities group and non-comorbidities group. We aimed to compare the clinical data, PAH-targeted strategies, and therapeutic responses between these two PAH groups. We further analyzed the impact of the numbers and categories of comorbidities on therapeutic responses.
Results: Almost half of the patients co-existed with cardiopulmonary diseases. Compared with non-comorbidities group (n = 40), comorbidities group (n = 36) were senior (p = 0.000) and male predominantly (p = 0.005). Comorbidities group also associated inconsistencies between hemodynamics and 6-min walking distance (6MWD), with a shorter 6MWD (p = 0.000), but a lower mean pulmonary artery pressure (mPAP) (p = 0.008). Non-comorbidities group showed an upturn in the WHO-FC (p = 0.010) and risk assessment (p = 0.033), while the improvement of hemodynamics [decreased mPAP (p = 0.009) and pulmonary vascular resistance (PVR) (p = 0.001), increased cardiac index (p = 0.001)] in comorbidities group did not match the change in clinical severity (no significant improvements in WHO-FC, risk stratification and 6MWD). When categorized by the comorbidities counts, it demonstrated that the more comorbidities, the more severe the clinical conditions, and the worse the therapeutic responses.
Conclusion: PAH patients with cardiopulmonary comorbidities represent a unique phenotype, with different clinical manifestation and treatment responses from typical PAH and inconsistencies between hemodynamics and functional status from baseline to follow-up.
Keywords: Clinical characteristics; Comorbidity; Pulmonary arterial hypertension (PAH); Therapeutic responses.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Informed consent of all participants was obtained for participation in the study. This study was approved by the Medical Ethics Committee of Beijing Anzhen Hospital Affiliated to Capital Medical University (KS2022037). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, Carlsen J, Coats AJS, Escribano-Subias P, Ferrari P, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43(38):3618–731. - PubMed
-
- Arvanitaki A, Vrana E, Boutsikou M, Anthi A, Apostolopoulou S, Avgeropoulou A, Demerouti E, Patrianakos A, Karyofyllis P, Mitrouska I, et al. The impact of cardiovascular comorbidities associated with risk for left heart disease on idiopathic pulmonary arterial hypertension: Data from the Hellenic Pulmonary Hypertension Registry (HOPE). Pulm Circ. 2022;12(2):e12086. - PMC - PubMed
-
- Hoeper MM, Huscher D, Ghofrani HA, Delcroix M, Distler O, Schweiger C, Grunig E, Staehler G, Rosenkranz S, Halank M, et al. Elderly patients diagnosed with idiopathic pulmonary arterial hypertension: results from the COMPERA registry. Int J Cardiol. 2013;168(2):871–80. - PubMed
-
- Frost AE, Badesch DB, Barst RJ, Benza RL, Elliott CG, Farber HW, Krichman A, Liou TG, Raskob GE, Wason P, et al. The changing picture of patients with pulmonary arterial hypertension in the United States: how REVEAL differs from historic and non-US Contemporary Registries. Chest. 2011;139(1):128–37. - PubMed
-
- Hjalmarsson C, Rådegran G, Kylhammar D, Rundqvist B, Multing J, Nisell MD, Kjellström B. Impact of age and comorbidity on risk stratification in idiopathic pulmonary arterial hypertension. Eur Respir J. 2018;51(5):1702310. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
