

Detection of cytomegalovirus in severely ill patients with intractable COVID-19; a retrospective study
- PMID: 40696312
- PMCID: PMC12281999
- DOI: 10.1186/s12889-025-23753-6
Detection of cytomegalovirus in severely ill patients with intractable COVID-19; a retrospective study
Abstract
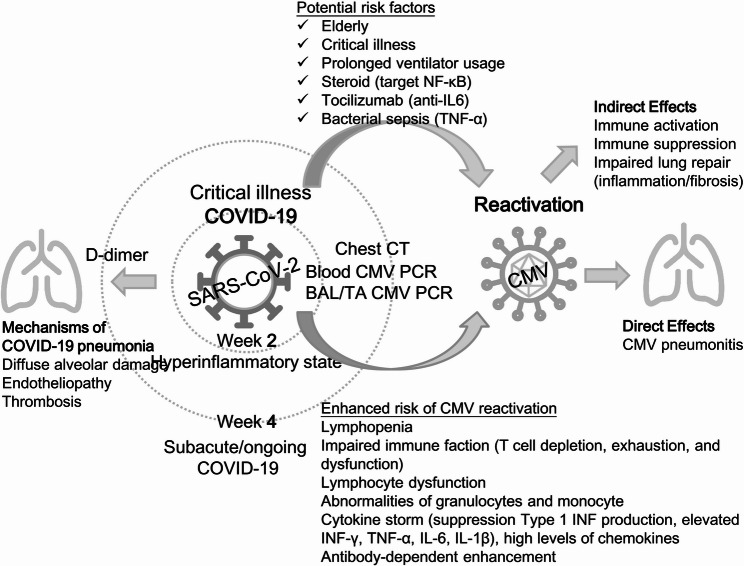
Objectives: We aimed to evaluate whether cytomegalovirus (CMV) reactivation affects the length of stay (LOS) and mortality of critically ill patients with coronavirus disease 2019 (COVID-19) following standard steroid and anti-cytokine treatments.
Study design: Retrospective data analysis of an observational cohort study.
Methods: We included all inpatients aged ≥ 20 years with severe acute respiratory syndrome coronavirus 2 infection in Northern Taiwan between May and July 2021. Blood, sputum, or endotracheal aspirate samples were collected weekly from critically ill patients with COVID-19 who did not respond to steroid treatment and sent for CMV reverse transcriptase-polymerase chain reaction testing. We investigated whether there were differences in comorbidities and prognoses between patients who tested positive for CMV and those who tested negative.
Results: Of the 167 inpatients with COVID-19, 43.3% (13/30) were critically ill, refractory to steroid treatment, and had CMV reactivation. Most (69.2%, 9/13) patients with CMV DNAemia had concurrent CMV positivity in the tracheal aspirate. Compared with CMV-negative patients, CMV-positive patients had a longer LOS but not higher 14- and 28-day mortality rates.
Conclusions: A high proportion of critically ill patients with COVID-19 who were refractory to steroid treatment developed CMV DNAemia. In critically ill patients with COVID-19, CMV reactivation can prolong hospitalization.
Keywords: COVID-19; Critically ill; Cytomegalovirus (CMV); Length of stay; Pneumonia; Steroid.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Institutional Review Board of Taipei City Hospital’s Ethics Committee approved this study (IRB No. TCHIRB-11008016-E). All patient data were anonymized and disconnected, with no minors included in the study. The IRB waived the requirement for written informed consent. Consent for publication: Not applicable. This study does not contain any individual person’s data in any form. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
