

Sub-phenotypes in patients with out-of-hospital cardiac arrest who undergo extracorporeal cardiopulmonary resuscitation: a retrospective observational study from a multicenter registry
- PMID: 40696402
- PMCID: PMC12281804
- DOI: 10.1186/s13054-025-05575-5
Sub-phenotypes in patients with out-of-hospital cardiac arrest who undergo extracorporeal cardiopulmonary resuscitation: a retrospective observational study from a multicenter registry
Abstract
Background: Out-of-hospital cardiac arrest (OHCA) has poor survival rates, but extracorporeal cardiopulmonary resuscitation (ECPR) shows promise for selected patients, as a second line of therapy after failure of conventional CPR to obtain return of spontaneous circulation, despite implementation challenges. This study aimed to identify distinct sub-phenotypes among patients with OHCA who undergo ECPR and to investigate their association with clinical outcomes.
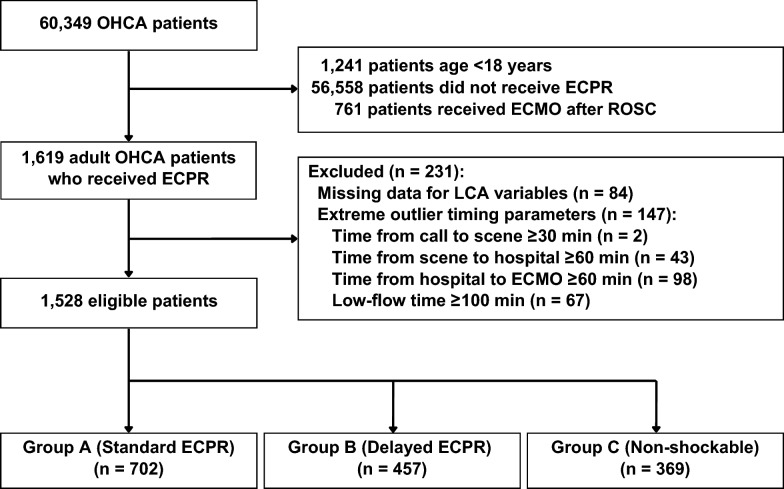
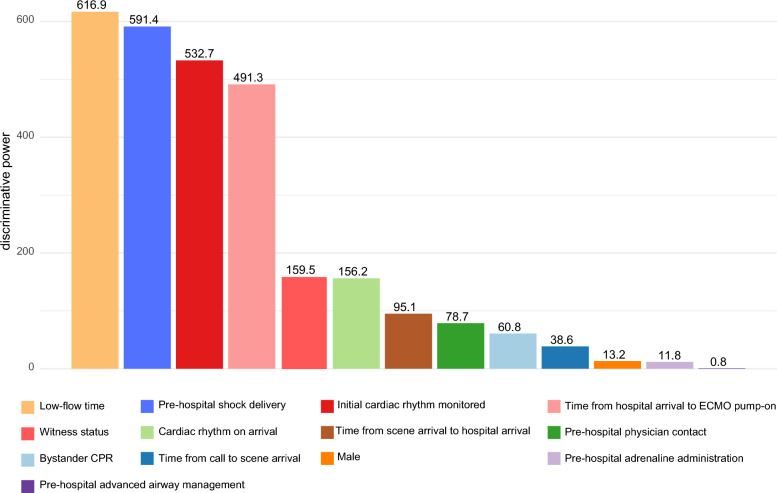
Methods: This multi-center, retrospective, observational study used the Japanese Association for Acute Medicine OHCA registry from 83 hospitals that performed ECPR among 91 participating centers between June 2014 and December 2020. We included adult patients with OHCA who received ECPR during cardiac arrest. Three-class latent class analysis (LCA) was employed to identify sub-phenotypes based on 15 variables, including pre- and in-hospital factors. Logistic regression analysis was used to assess the association between sub-phenotypes and 30-day survival and neurological outcomes.
Results: A total of 1528 patients were included. The median low-flow time was 47 min (interquartile rage: 38-58 min). The 30-day survival rate for eligible patients was 20.9%. LCA identified three distinct sub-phenotypes: Standard ECPR Group (n = 702), Delayed ECPR Group (n = 457), and Non-shockable Rhythm Group (n = 369). The variables with high discriminative power in the LCA was low-flow time, followed by pre-hospital shock delivery and initial cardiac rhythm. Thirty-day survival rates varied significantly among the sub-phenotypes (p = 0.001): Standard ECPR Group (26.9%), Delayed ECPR Group (17.1%), and Non-shockable Rhythm Group (14.1%). Favorable neurological outcomes at 30 days also differed significantly (p = 0.004), with the Standard ECPR Group showing the highest rate (12.1%). After adjusting for covariates, both the Delayed ECPR Group (adjusted OR: 0.61, 95% CI 0.44-0.82) and Non-shockable Rhythm Group (adjusted OR: 0.47, 95% CI 0.32-0.68) had significantly lower odds of 30-day survival compared to the Standard ECPR Group.
Conclusions: Three clinically meaningful sub-phenotypes were identified using simple pre-hospital and in-hospital factors, with low-flow time emerging as the most critical discriminating factor. The sub-phenotypes showed significant associations with clinical outcomes and provide a practical framework for ECPR patient stratification. These findings suggest that timing optimization may be as important as rhythm characteristics for ECPR patient selection and support the development of sub-phenotype-specific treatment strategies.
Keywords: Cardiac arrest; Extracorporeal cardiopulmonary resuscitation; Latent class analysis; Sub-phenotype.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The registry protocol was approved by the Institutional Review Board of each participating hospital. The participating hospitals are listed on the JAAM-OHCA website [28]. The requirement for informed consent was waived because the observational study design minimized risk to patients and preserved anonymity. Patients and their respective families were allowed to opt-out of the registry. The institutional research ethics committee of Jichi Medical University Saitama Medical Center approved the present study (S19-016). Consent for publication: Not applicable. No individual patient data will be reported. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Extracorporeal and Conventional Cardiopulmonary Resuscitation and Low-Flow Duration: Insights From a Nationwide Hospital-Based Registry Study in Japan (JAAM-OHCA Registry).J Am Heart Assoc. 2025 Jul 15;14(14):e039938. doi: 10.1161/JAHA.124.039938. Epub 2025 Jul 14. J Am Heart Assoc. 2025. PMID: 40654244
-
Prognostic effects of cardiopulmonary resuscitation (CPR) start time and the interval between CPR to extracorporeal cardiopulmonary resuscitation (ECPR) on patient outcomes under extracorporeal membrane oxygenation (ECMO): a single-center, retrospective observational study.BMC Emerg Med. 2024 Mar 5;24(1):36. doi: 10.1186/s12873-023-00905-8. BMC Emerg Med. 2024. PMID: 38438853 Free PMC article.
-
Waveform conversion as a prognostic factor of poor prognosis in patients undergoing extracorporeal cardiopulmonary resuscitation.Am J Emerg Med. 2025 Jul;93:103-108. doi: 10.1016/j.ajem.2025.03.041. Epub 2025 Mar 30. Am J Emerg Med. 2025. PMID: 40179822
-
Continuous chest compression versus interrupted chest compression for cardiopulmonary resuscitation of non-asphyxial out-of-hospital cardiac arrest.Cochrane Database Syst Rev. 2017 Mar 27;3(3):CD010134. doi: 10.1002/14651858.CD010134.pub2. Cochrane Database Syst Rev. 2017. PMID: 28349529 Free PMC article.
-
Prognostic factors associated with favourable functional outcome among adult patients requiring extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest: A systematic review and meta-analysis.Resuscitation. 2023 Dec;193:110004. doi: 10.1016/j.resuscitation.2023.110004. Epub 2023 Oct 18. Resuscitation. 2023. PMID: 37863420
References
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–639. - PubMed
-
- Holmberg MJ, Granfeldt A, Guerguerian AM, Sandroni C, Hsu CH, Gardner RM, Lind PC, Eggertsen MA, Johannsen CM, Andersen LW. Extracorporeal cardiopulmonary resuscitation for cardiac arrest: an updated systematic review. Resuscitation. 2023;182: 109665. - PubMed
-
- Low CJW, Ramanathan K, Ling RR, Ho MJC, Chen Y, Lorusso R, MacLaren G, Shekar K, Brodie D. Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with cardiac arrest: a comparative meta-analysis and trial sequential analysis. Lancet Respir Med. 2023;11(10):883–93. - PubMed
-
- Yannopoulos D, Bartos J, Raveendran G, Walser E, Connett J, Murray TA, Collins G, Zhang L, Kalra R, Kosmopoulos M, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020;396(10265):1807–16. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
