

The Mathematics of Serocatalytic Models With Applications to Public Health Data
- PMID: 40696544
- PMCID: PMC12284347
- DOI: 10.1002/sim.70188
The Mathematics of Serocatalytic Models With Applications to Public Health Data
Abstract
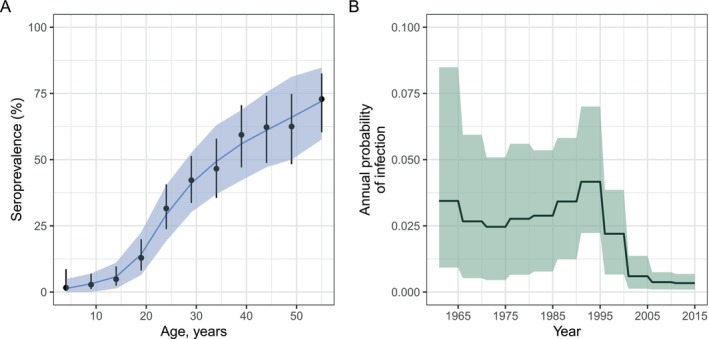
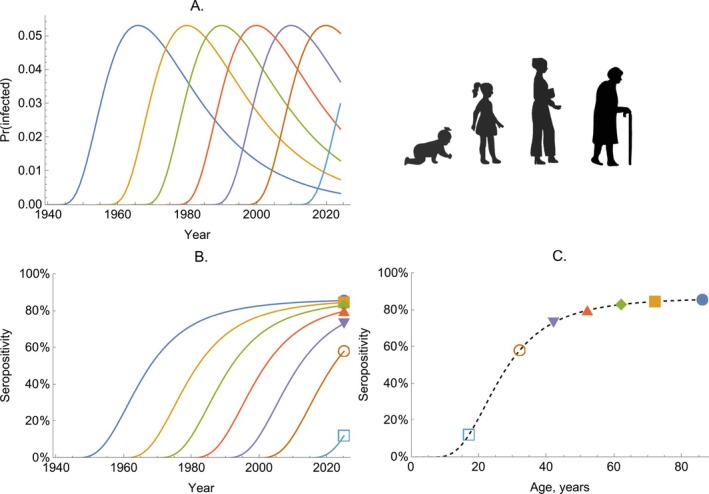
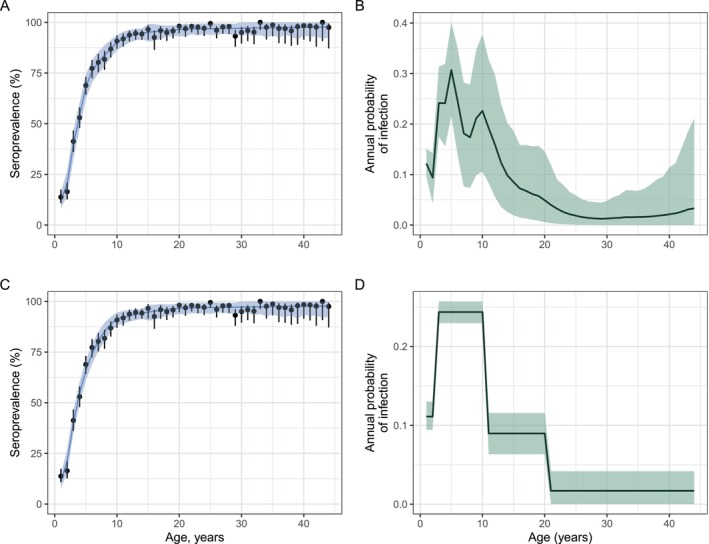
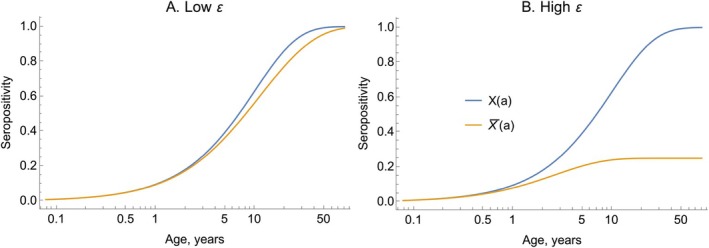
Serocatalytic models are powerful tools which can be used to infer historical infection patterns from age-structured serological surveys. These surveys are especially useful when disease surveillance is limited and have an important role to play in providing a ground truth gauge of infection burden. In this tutorial, we consider a wide range of serocatalytic models to generate epidemiological insights. With mathematical analysis, we explore the properties and intuition behind these models and include applications to real data for a range of pathogens and epidemiological scenarios. We also include practical steps and code in R and Stan for interested learners to build experience with this modeling framework. Our work highlights the usefulness of serocatalytic models and shows that accounting for the epidemiological context is crucial when using these models to understand infectious disease epidemiology.
© 2025 The Author(s). Statistics in Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Muench H., “Derivation of Rates From Summation Data by the Catalytic Curve,” Journal of the American Statistical Association 29 (1934): 25–38.
-
- Cutts F. T. and Hanson M., “Seroepidemiology: An Underused Tool for Designing and Monitoring Vaccination Programmes in Low‐and Middle‐Income Countries,” Tropical Medicine & International Health 21 (2016): 1086–1098. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources