

Comparison of prognostic factors and their differences in intrahepatic, hilar, and distal cholangiocarcinoma: A systematic review and meta-analysis
- PMID: 40697248
- PMCID: PMC12278260
- DOI: 10.4251/wjgo.v17.i7.107995
Comparison of prognostic factors and their differences in intrahepatic, hilar, and distal cholangiocarcinoma: A systematic review and meta-analysis
Abstract
Background: Cholangiocarcinoma (CCA) comprises heterogeneous malignancies arising at different anatomical locations: Intrahepatic cholangiocarcinoma (IHCC), perihilar cholangiocarcinoma (PHCC), and distal cholangiocarcinoma (DCC). These subtypes exhibit distinct clinical behaviors, treatment approaches, and outcomes. Despite advances in surgical and adjuvant therapies, the prognostic implications of tumor location remain unclear and inconsistently reported. Understanding these variations is essential for personalized management and staging refinement. We hypothesized that the anatomical subtype of CCA significantly influences prognostic outcomes and pathological features.
Aim: To compare prognostic outcomes and clinicopathological characteristics among IHCC, PHCC, and DCC based on current evidence.
Methods: A systematic review and meta-analysis were conducted in accordance with PRISMA guidelines. PubMed, EMBASE, and the Cochrane Library were searched, yielding 11 eligible retrospective comparative studies involving 14484 patients (IHCC: 6260; PHCC: 6895; DCC: 1329). Outcomes assessed included overall survival (OS), lymph node metastasis, neural invasion, and vascular invasion. Statistical analyses were performed using RevMan 5.3 and Stata 13.0.
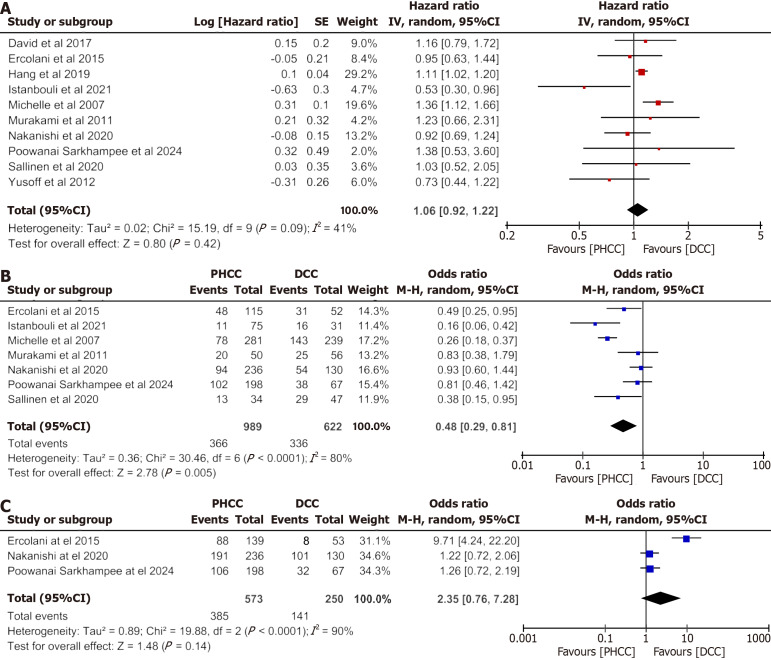
Results: DCC demonstrated the most favorable prognosis among all subtypes. Despite the highest lymph node metastasis rate (DCC: 56.9%), it was associated with better OS than PHCC and IHCC. Vascular invasion was more prevalent in IHCC (OR = 1.66, 95%CI: 1.22-2.28, P = 0.001). OS comparisons showed no significant difference between PHCC and IHCC (HR = 1.02, P = 0.88), while DCC showed consistent trends toward better survival against both.
Conclusion: Anatomical subtype is a significant prognostic factor in CCA. DCC patients experience superior outcomes despite aggressive lymphatic spread, suggesting better resectability and surgical outcomes. These insights underscore the need for subtype-specific management strategies and future prospective validation.
Keywords: Cholangiocarcinoma; Distal; Intrahepatic; Lymph node metastasis; Meta-analysis; Perihilar; Prognosis; Survival.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declared no conflict of interest.
Figures



References
-
- Menon G, Garikipati SC, Roy P. Cholangiocarcinoma. 2024 May 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan- - PubMed
LinkOut - more resources
Full Text Sources
