

doi: 10.1016/j.xrrt.2025.02.003.
eCollection 2025 Aug.
Long head of the biceps as a local autograft for surgical treatment of high-grade acromioclavicular dislocations: a clinical anatomy and feasibility study
Affiliations
- PMID: 40697291
- PMCID: PMC12277751
- DOI: 10.1016/j.xrrt.2025.02.003
Item in Clipboard
Long head of the biceps as a local autograft for surgical treatment of high-grade acromioclavicular dislocations: a clinical anatomy and feasibility study
JSES Rev Rep Tech.
.
No abstract available
Keywords: Acromioclavicular dislocation; Acromioclavicular ligamentoplasty; Autograft; Chronic dislocation; Clinical anatomy study; Long head of the biceps; Surgical treatment.
Figures

The patient is placed in the beach chair position with the affected limb at the side, optionally held by a mechanical arm holder.
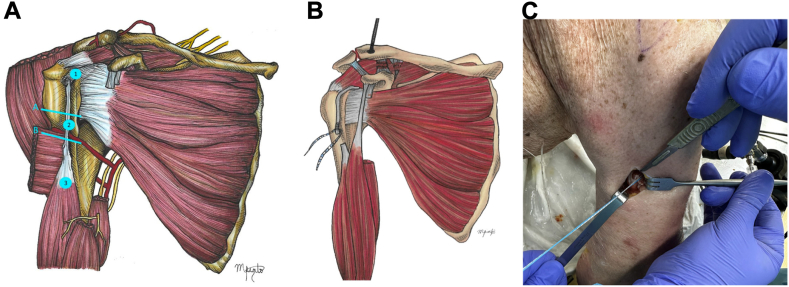
LHB tenotomy and subpectoral tenodesis: (A) The LHB is tenotomized 1 cm proximal to the myotendinous junction (near zone 3 in this image). (B) The proximal stump of the LHB graft was rerouted proximally, maintaining its original insertion into the supraglenoid tubercle and superior labrum. (C) The distal stump of LHB is tenodesed with an all-suture anchor (Y-Knot RC 2.8 mm; Conmed, Largo, FL, USA). LHB, long head of the biceps.
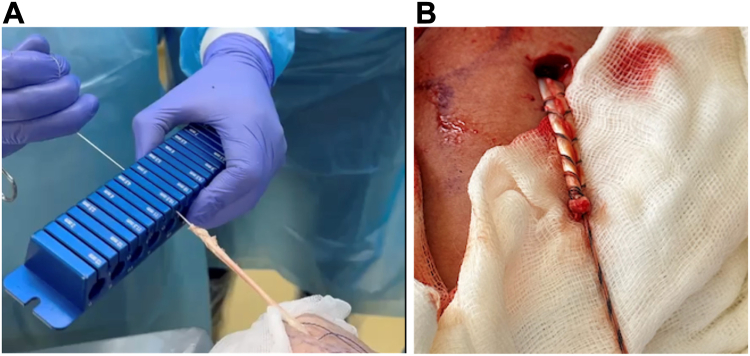
LHB graft preparation: (A) The proximal stump of the LHB graft is rerouted proximally, maintaining its original insertion in the supraglenoid tubercle and superior labrum, and retrieved through the RI. The tendon diameter is verified using a calibrated sizer and trimmed to 4-4.5 cm. (B) The prepared tendon was then secured with two sutures in a Krackow fashion. LHB, long head of the bicep; RI, rotator interval.
Coracoclavicular (CC) tunnel: A 4.5 mm tunnel is drilled, connecting the superior border of the clavicle (3.5 cm medial to the AC joint) and exiting at the inferior border of the coracoid process using a drill guide. A 2.4 mm guide wire is then passed, ideally at the midpoint of the coracoid process, and fluoroscopic confirmation is obtained before creating the tunnel with a 4.5 mm drill. AC, acromioclavicular.
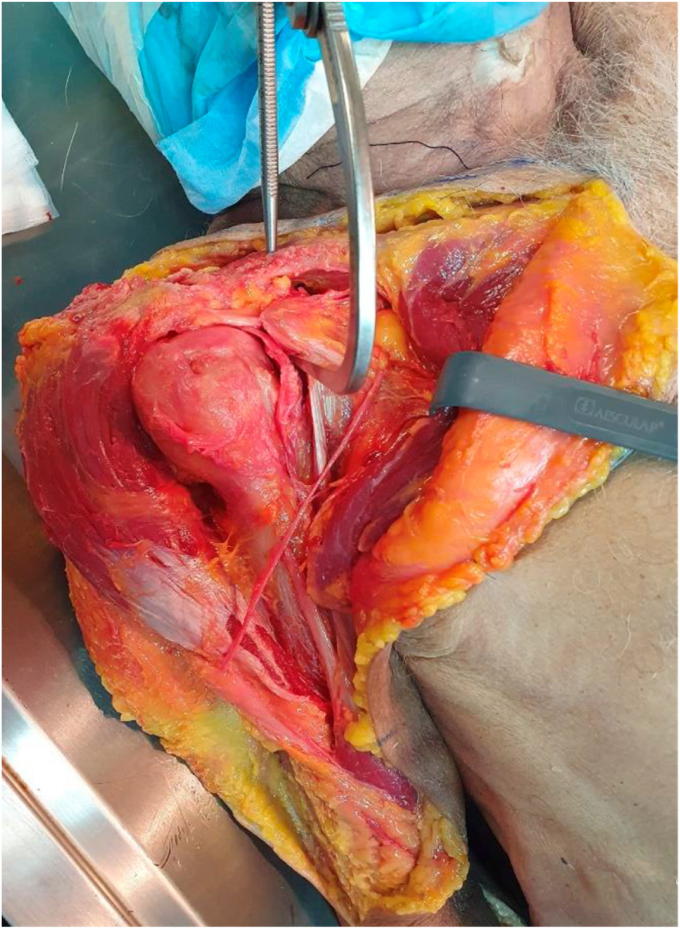
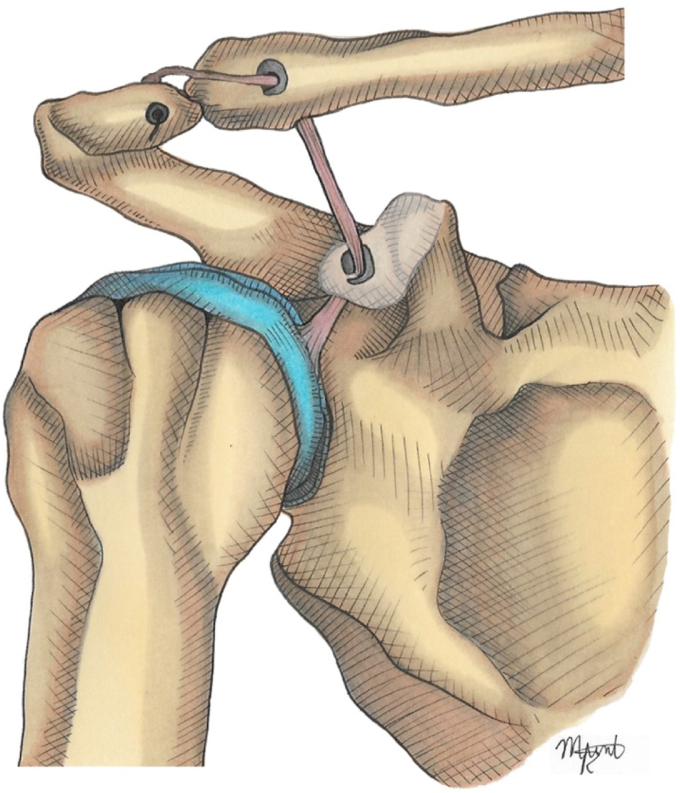
CC graft passage and fixation: A suture passer is used to shuttle both suture strands, holding the free end of the tendon and suspensory system through the tunnel. The AC joint was reduced, and the system was locked with the superior button apposed to the upper border of the clavicle, providing vertical stability. CC, coracoclavicular; AC, acromioclavicular.
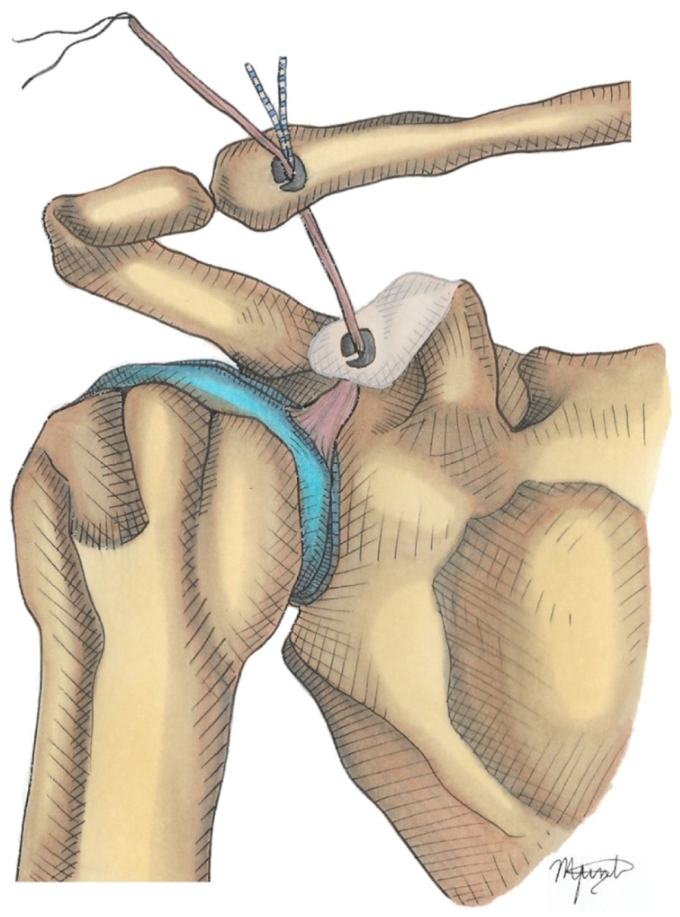
Acromion tunnel and fixation: 1 cm laterally to the AC joint, a 3 mm tunnel parallel to the joint line is drilled in the acromion. The remaining LHB tendon is passed from posterior to anterior and fixed using a Knotless anchor. If possible, the AC joint posterosuperior ligament and capsule are reinforced with side-to-side stitches to the graft. LHB, long head of the bicep; AC, acromioclavicular.
Similar articles
-
Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults.Cochrane Database Syst Rev. 2010 Aug 4;2010(8):CD007429. doi: 10.1002/14651858.CD007429.pub2. Cochrane Database Syst Rev. 2010. PMID: 20687087 Free PMC article.
-
Operative versus non-operative management following Rockwood grade III acromioclavicular separation: a meta-analysis of the current evidence base.J Orthop Traumatol. 2011 Mar;12(1):19-27. doi: 10.1007/s10195-011-0127-1. Epub 2011 Feb 23. J Orthop Traumatol. 2011. PMID: 21344264 Free PMC article.
-
Long Head of Biceps Tendinopathy Is Associated With Age and Cuff Tendinopathy on MRI Obtained for Evaluation of Shoulder Pain.Clin Orthop Relat Res. 2025 May 1;483(5):869-877. doi: 10.1097/CORR.0000000000003342. Epub 2024 Dec 12. Clin Orthop Relat Res. 2025. PMID: 39679662
-
Surgical versus conservative management of Type III acromioclavicular dislocation: a systematic review.Br Med Bull. 2017 Jun 1;122(1):31-49. doi: 10.1093/bmb/ldx003. Br Med Bull. 2017. PMID: 28334148
-
Acromioclavicular Fixation Before Coracoclavicular Tunnel Placement and Acromioclavicular Construct Design Improved Reduction and Stability in a Whole-Shoulder Girdle Model: A Pilot Study.Am J Sports Med. 2025 Jul;53(9):2041-2051. doi: 10.1177/03635465251349143. Epub 2025 Jun 26. Am J Sports Med. 2025. PMID: 40566939 Free PMC article.
References
-
- Beitzel K., Mazzocca A.D., Bak K., Itoi E., Kibler W.B., Mirzayan R., et al. ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy. 2014;30:271–278. doi: 10.1016/j.arthro.2013.11.005. - DOI - PubMed
LinkOut - more resources
Full Text Sources
