

The Effects of Transcranial Direct Current Stimulation During Extended Reality Exercises for Cortical, Neuromuscular, and Clinical Recovery of Stroke Survivors
- PMID: 40697356
- PMCID: PMC12283194
- DOI: 10.1155/np/5688648
The Effects of Transcranial Direct Current Stimulation During Extended Reality Exercises for Cortical, Neuromuscular, and Clinical Recovery of Stroke Survivors
Abstract
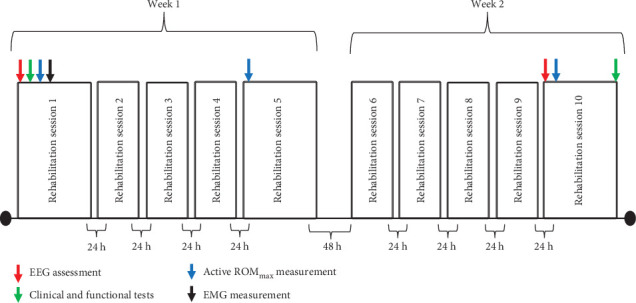
Background: Rehabilitation methods that include anodal transcranial direct current stimulation (atDCS) and extended reality (XR) exercises have been used to enhance neural networks and improve functional performance in stroke patients, but the neuromuscular and neurophysiological mechanisms underlying these improvements are not fully understood. The purpose of this study was to examine the effects of atDCS during XR rehabilitation exercises on cortical, neuromuscular, and clinical outcomes of stroke survivors. Methods: Nineteen chronic stroke survivors were placed into either a transcranial direct current stimulation (tDCS) or a Sham group, without significant (p > 0.73) differences in the baseline levels of disability between groups. The tDCS group received active atDCS and the Sham group received sham atDCS applied on the ipsilesional primary motor cortex (M1) while performing a 10-session XR rehabilitation program. Surface electromyography (EMG) activity was recorded from deltoid and rectus femoris of the paretic limb without and with the application of active/sham atDCS on the M1. Shoulder abduction and hip flexion active maximum joint range of motion (ROMmax), electroencephalography (EEG)-derived brain symmetry index (BSI) and functional/clinical tests were assessed before and after the rehabilitation program. Results: EMG activity was ~ 31% greater during hip flexion of the paretic limb with the application of active atDCS than without atDCS (p=0.04). Paretic hip flexion ROMmax increased by ~ 26%, BSI decreased by ~ 72% (indicating greater brain symmetry) and timed up and go (TUG) functional test improved by ~ 11% from before to after the rehabilitation program for the tDCS group only (p < 0.05). No other significant differences (p > 0.05) were observed. Conclusion: It seems that the application of active atDCS targeted the ipsilesional M1 representation of the quadriceps, which potentiated muscle activation in the paretic rectus femoris during XR exercises and resulted in greater motor recovery in hip flexion movements. The EEG-derived BSI results also indicate that atDCS was effective in reorganizing the ipsilesional hemisphere brain activity after stroke.
Keywords: electroencephalography; electromyography activity; extended reality; functional recovery; transcranial direct current stimulation.
Copyright © 2025 Cassio V. Ruas et al. Neural Plasticity published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





References
-
- Shani S. D., Varma R. P., Sarma P. S., Sylaja P. N., Kutty V. R. Life Style and Behavioural Factors are Associated With Stroke Recurrence Among Survivors of First Episode of Stroke: A Case Control Study. Journal of Stroke and Cerebrovascular Diseases . 2021;30(4) doi: 10.1016/j.jstrokecerebrovasdis.2021.105606.105606 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
