

Systemic immune-inflammation index and systemic inflammation response index levels are associated with coronary heart disease prevalence in the asthmatic population: a cross-sectional analysis of the NHANES 2011-2018
- PMID: 40697833
- PMCID: PMC12279799
- DOI: 10.3389/fpubh.2025.1514016
Systemic immune-inflammation index and systemic inflammation response index levels are associated with coronary heart disease prevalence in the asthmatic population: a cross-sectional analysis of the NHANES 2011-2018
Abstract
Background: Earlier studies have indicated a positive correlation systemic immune-inflammatory index (SII) and systemic inflammatory response index (SIRI) levels and the development of coronary heart disease (CHD). However, the correlation between SII, SIRI levels and the incidence of CHD in patients with asthma has not been described. The purpose of the study was to research the potential correlation between the levels of SII, SIRI and the incidence of CHD in patients with asthma.
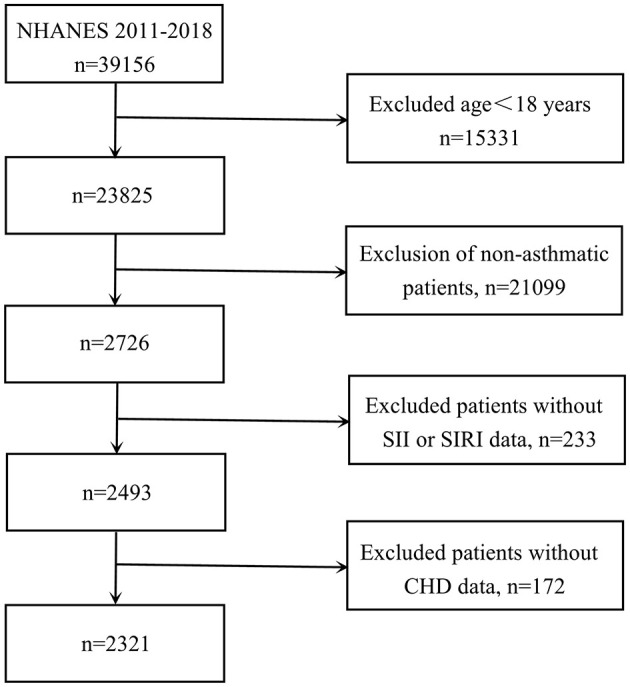
Methods: We conducted a retrospective cross-sectional analysis in which data of individuals from the National Health and Nutrition Examination Survey (NHANES) between 2011 and 2018. This study included 39,156 adults. Weighted multivariable regression analysis and subgroup analyses were used to assess the independent and combined associations between CHD prevalence and SII, SIRI levels of asthmatic population.
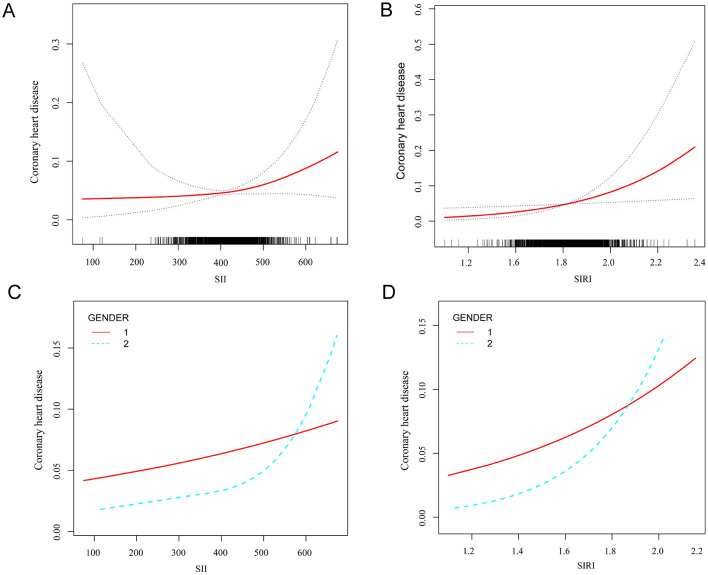
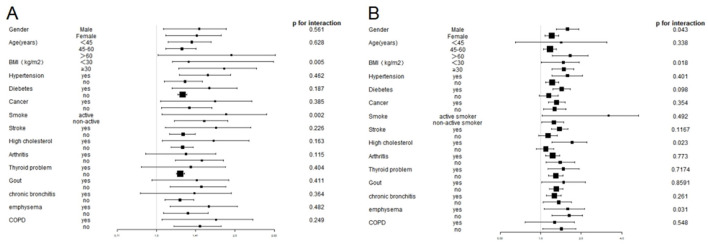
Results: Totally, 2,321 adults were included in our analysis, with 116 participants experiencing CHD and the remaining 2,205 participants being free of CHD. SII levels did not significantly correlate with any of the participants' baseline characteristics, nor did SIRI levels (r < 0.1). Higher levels of SII were related to increased incidence of CHD, with an OR of 1.462 (95% CI, 1.031-1.893) (p < 0.001). Similarly, SIRI levels had similar results, with OR of 1.268 (95% CI, 1.095-1.441) (p < 0.05). Positive correlations between SII, SIRI levels and the incidence of CHD were observed (p < 0.05). Curve fitting further illustrated a positive correlation between SII, SIRI and the incidence of CHD in participants with asthma. Threshold effect analysis showed that higher levels of SII and SIRI were associated with a higher incidence of CHD, especially when SII and SIRI levels exceeded the thresholds of 411.238 and 1.812. Stratified analyses confirmed that the associations between higher SII and SIRI and increased CHD incidence in most subgroups remained consistent.
Conclusions: The incidence of CHD in asthmatic individuals was positively correlated with elevated SII and SIRI levels among US adults. SII and SIRI serve as recently emerged inflammatory markers for assessing CHD prevalence in the asthmatic population. However, in order to confirm these findings, more rigorous large-scale prospective studies are needed.
Keywords: NHANES; asthma; coronary heart disease; systemic immune-inflammation index; systemic inflammation response index.
Copyright © 2025 Wu, Zhang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Soriano JB, Abajobir AA, Abate KH, Abera SF, Agrawal A, Ahmed MB et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. (2017) 5:691–706. 10.1016/S2213-2600(17)30293-X - DOI - PMC - PubMed
-
- Asthma GIF. 2017 GINA report: global strategy for asthma management and prevention. (2024). Available online at: http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-managem...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical