

Lp(a) in daily clinical routine: risk-factor for both cardiovascular events and heart-failure? A retrospective analysis of the Luebeck Lp(a) heart-failure (HF) registry in patients after myocardial infarction
- PMID: 40697899
- PMCID: PMC12281520
- DOI: 10.1016/j.athplu.2025.07.002
Lp(a) in daily clinical routine: risk-factor for both cardiovascular events and heart-failure? A retrospective analysis of the Luebeck Lp(a) heart-failure (HF) registry in patients after myocardial infarction
Abstract
Background and aims: Atherosclerotic cardiovascular disease (ASCVD) is a major health burden being the leading cause of death in Europe. Lipoprotein (a) (Lp(a)) is an important risk factor for CV events reflected by the 2019 ESC recommendation of a once in a lifetime Lp(a) measurement. Furthermore, heart-failure (HF) is the number one diagnosis for hospital admission in Germany and Europe. HF and ASCVD share common well-known risk factors, e.g. diabetes, obesity and hypertension. So far, there is scarcity of data regarding the relationship between Lp(a) and HF. We hypothesized that Lp(a) might be elevated in a high-risk ASCVD patient collective and that there might also be an association with heart-failure.
Methods: The Luebeck Lp(a) HF registry is a combined retrospective/prospective single-center, all-comers registry which investigates the relationship between Lp(a) and HF. The retrospective analysis reported here, comprises patients who were admitted to our heart-catheterization laboratory in the year 2021 due to ST-segment elevation myocardial infarction (STEMI) or non-ST-segment elevation myocardial infarction (NSTEMI).
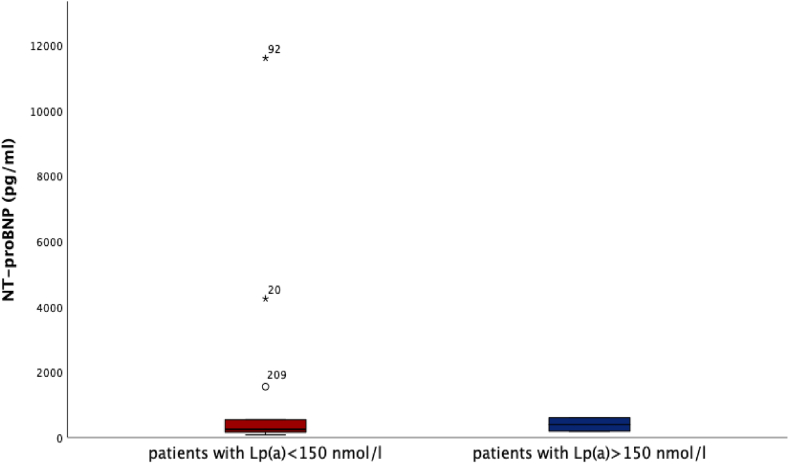
Results: We found that Lp(a) was assessed only in a minority of patients presenting with STEMI (33 %) and NSTEMI (14.6 %), p < 0.001. There was no relationship between Lp(a) level and ejection fraction (EF) or NTproBNP as surrogate markers for HF, respectively. Statin pretreatment was more frequent in patients with NSTEMI (31.1 %) compared to STEMI patients (11.3 %), p < 0.001.
Conclusion: Despite ESC recommendation, routine Lp(a) measurement is only rarely performed even in a high-risk patient collective. In patients with MI, we could retrospectively not observe a correlation between Lp(a) levels and heart failure, as assessed by surrogate markers as EF and NTproBNP.
Keywords: Heart-failure; Lp(a); Myocardial infarction; Pelacarsen.
© 2025 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Townsend N., et al. Cardiovascular disease in Europe — epidemiological update 2015. Eur Heart J. 2015;36(40):2696–2705. - PubMed
-
- Welsh P., et al. Elevated lipoprotein(a) increases risk of subsequent major adverse cardiovascular events (MACE) and coronary revascularisation in incident ASCVD patients: a cohort study from the UK biobank. Atherosclerosis. 2024;389 - PubMed
-
- Mach F., et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and european atherosclerosis society (EAS) Eur Heart J. 2020;41(1):111–188. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous