

A comparative analysis of non-invasive respiratory support modalities in the treatment of acute hypercapnic respiratory failure: a network meta-analysis
- PMID: 40697918
- PMCID: PMC12279498
- DOI: 10.3389/fmed.2025.1594128
A comparative analysis of non-invasive respiratory support modalities in the treatment of acute hypercapnic respiratory failure: a network meta-analysis
Abstract
Aim: The purpose of this study is to compare different non-invasive respiratory support methods for the treatment of acute hypercapnic respiratory failure (AHRF).
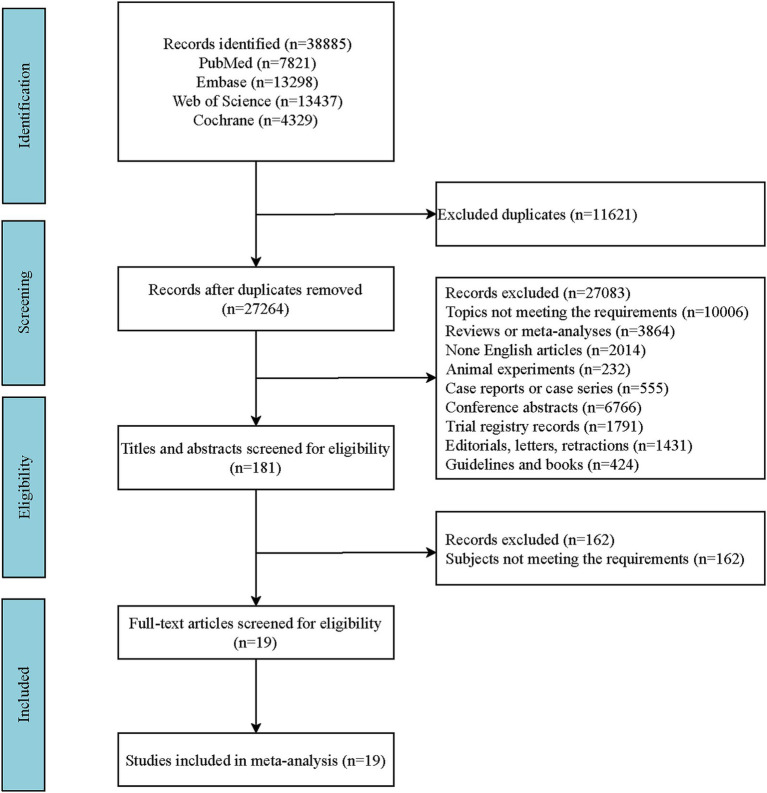
Methods: The network meta-analysis was conducted based on studies from PubMed, Embase, the Cochrane Library, and Web of Science, from their inception to September 10, 2024. The outcomes was treatment failure, all-cause mortality, intubation, dyspnea score, length of stay in hospital, respiratory rate, arterial carbon dioxide partial pressure (PaCO2), and complications. The results of both direct and indirect comparisons were quantitatively assessed using weighted mean differences or relative risks with their respective 95% confidence intervals, and graphically depicted in forest plots. Additionally, the rank probabilities were presented, demonstrating the likelihood of each non-invasive respiratory support method being the most effective across various measured outcomes.
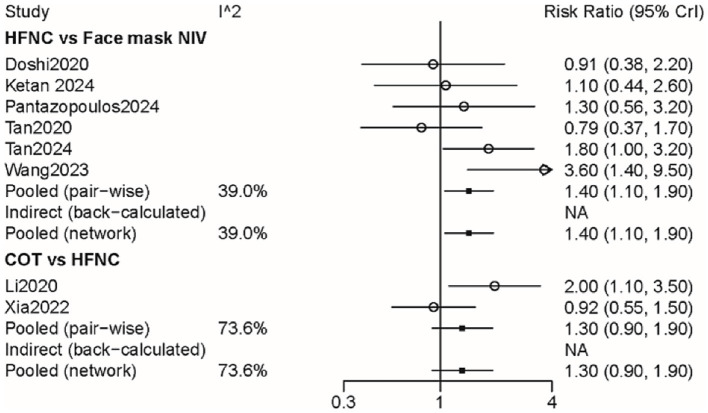
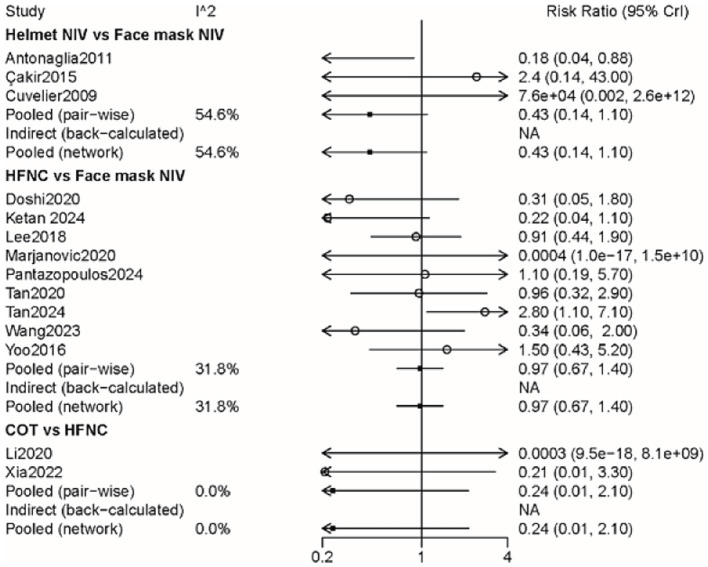
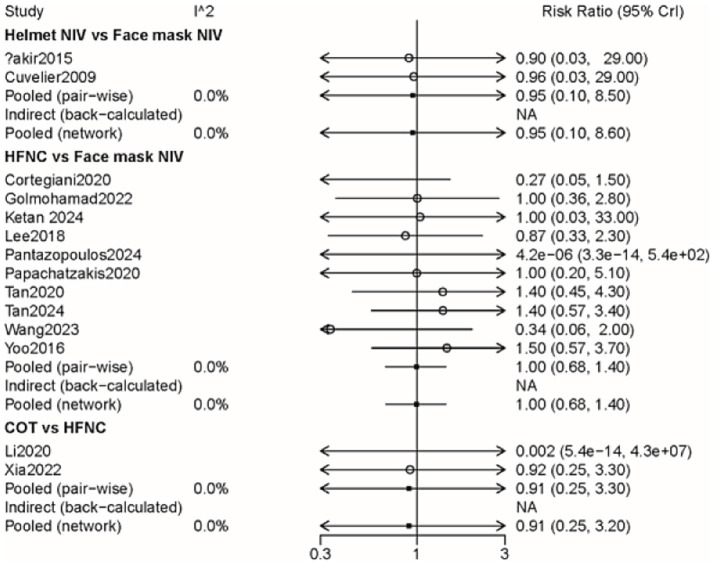
Results: Nineteen studies (2,022 participants) were included. The results indicated that the probability of treatment failure with face mask non-invasive ventilation (NIV) was lower than that of high-flow nasal cannula (HFNC) (RR: 1.42, 95% CI: 1.06, 1.93) and conventional oxygen treatment (COT) (RR: 1.87, 95% CI: 1.16, 3.03). Face mask NIV demonstrated superior performance in dyspnea score and PaCO2 compared to HFNC, helmet NIV, and COT. The length of stay in the hospital for face mask NIV was relatively longer compared to HFNC (WMD: -0.73, 95% CI: -1.35, -0.10) and COT (WMD: -1.09, 95% CI: -2.00, -0.18), and the probability of complications was higher than with HFNC. The rank probability suggested that COT had the lowest likelihood of intubation and all-cause mortality, while helmet NIV may have the best effect on improving respiratory rate.
Conclusion: Concerning treatment failure, dyspnea score, and PaCO2 improvement in patients with AHRF, face mask NIV may outperform other methods. For selected patients with AHRF, face mask NIV might be considered for potential first-line method. This study provides a certain level of evidence-based support for the management and treatment of AHRF, but more research is still needed in the future to determine the optimal non-invasive respiratory support method for treating patients with AHRF. In clinic, the efficacy of face mask NIV for better outcomes in patients with AHRH still requires validation.
Keywords: acute hypercapnic respiratory failure; conventional oxygen treatment; high-flow nasal cannula; non-invasive respiratory support; non-invasive ventilation.
Copyright © 2025 Yan and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2017 Jul 13;7(7):CD004104. doi: 10.1002/14651858.CD004104.pub4. Cochrane Database Syst Rev. 2017. PMID: 28702957 Free PMC article.
-
High flow nasal cannula for respiratory support in term infants.Cochrane Database Syst Rev. 2023 Aug 4;8(8):CD011010. doi: 10.1002/14651858.CD011010.pub2. Cochrane Database Syst Rev. 2023. PMID: 37542728 Free PMC article.
-
Chronic non-invasive ventilation for chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2021 Aug 9;8(8):CD002878. doi: 10.1002/14651858.CD002878.pub3. Cochrane Database Syst Rev. 2021. PMID: 34368950 Free PMC article.
-
High-flow nasal cannulae for respiratory support in adult intensive care patients.Cochrane Database Syst Rev. 2017 May 30;5(5):CD010172. doi: 10.1002/14651858.CD010172.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2021 Mar 4;3:CD010172. doi: 10.1002/14651858.CD010172.pub3. PMID: 28555461 Free PMC article. Updated.
-
High flow nasal cannula versus conventional oxygen therapy and non-invasive ventilation in adults with acute hypoxemic respiratory failure: A systematic review.Respir Med. 2016 Dec;121:100-108. doi: 10.1016/j.rmed.2016.11.004. Epub 2016 Nov 3. Respir Med. 2016. PMID: 27888983
References
-
- Xu C, Yang F, Wang Q, Gao W. Comparison of high flow nasal therapy with non-invasive ventilation and conventional oxygen therapy for acute hypercapnic respiratory failure: a meta-analysis of randomized controlled trials. Int J Chron Obstruct Pulmon Dis. (2023) 18:955–73. doi: 10.2147/copd.S410958, PMID: - DOI - PMC - PubMed
-
- van Beek JHGM. Effects of hypoxia and hypercapnia on cardiac contractility and energetics In: Physiology and pharmacology of cardio-respiratory control. Dordrecht: Springer; (1998). 19–24.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous