

Frontal QRS-T angle remains unchanged in fibromyalgia: a cross-sectional study with implications for routine ECG screening
- PMID: 40697924
- PMCID: PMC12279751
- DOI: 10.3389/fmed.2025.1615561
Frontal QRS-T angle remains unchanged in fibromyalgia: a cross-sectional study with implications for routine ECG screening
Abstract
Aim: Fibromyalgia syndrome (FMS) is a chronic condition characterized by widespread pain and associated with systemic diseases. Although autonomic dysfunction in FMS may predispose to cardiac arrhythmias, its impact on cardiac parameters, such as the frontal QRS-T [f(QRS-T)] angle, remains unclear. This study aimed to investigate the f(QRS-T) angle in FMS patients compared to healthy controls.
Methods: A total of 75 FMS patients and 75 healthy controls were included in this cross-sectional study. Disease severity was assessed using the Fibromyalgia Impact Questionnaire (FIQ). The f(QRS-T) angle was calculated from 12-lead electrocardiograms by a blinded cardiologist. Associations between the f(QRS-T) angle, FIQ scores, and duloxetine use were analyzed using appropriate statistical methods.
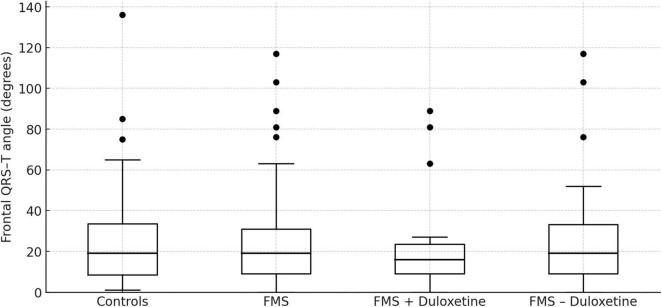
Results: No significant differences in the f(QRS-T) angle were observed between FMS patients and controls (p = 0.973). Additionally, no correlation was found between FIQ scores and the f(QRS-T) angle (p = 0.725). Subgroup analysis revealed no significant differences in the f(QRS-T) angle between FMS patients using duloxetine and those not using it (p = 0.503).
Conclusion: Contrary to concerns about subclinical cardiac involvement in FMS, our findings reveal no significant alterations in the f(QRS-T) angle among FMS patients. Moreover, disease severity and duloxetine use do not influence this parameter. These results challenge the assumption of clinically relevant cardiac dysregulation in FMS and suggest that routine ECG screening may not be necessary for patients with FMS. Nonetheless, longitudinal studies are warranted to fully clarify the long-term cardiac risk in this population.
Keywords: arrhythmia; autonomic dysfunction; cardiac screening; chronic pain; duloxetine; electrocardiogram; fibromyalgia; frontal QRS-T angle.
Copyright © 2025 Tezcan and Tezcan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
-
Serotonin and noradrenaline reuptake inhibitors (SNRIs) for fibromyalgia.Cochrane Database Syst Rev. 2018 Feb 28;2(2):CD010292. doi: 10.1002/14651858.CD010292.pub2. Cochrane Database Syst Rev. 2018. PMID: 29489029 Free PMC article.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Transcutaneous electrical nerve stimulation (TENS) for fibromyalgia in adults.Cochrane Database Syst Rev. 2017 Oct 9;10(10):CD012172. doi: 10.1002/14651858.CD012172.pub2. Cochrane Database Syst Rev. 2017. PMID: 28990665 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
LinkOut - more resources
Full Text Sources
Miscellaneous