

Types of Myocardial Infarction in People With HIV in Switzerland
- PMID: 40698031
- PMCID: PMC12282347
- DOI: 10.1093/ofid/ofaf357
Types of Myocardial Infarction in People With HIV in Switzerland
Abstract
Background: Of myocardial infarctions (MIs) recorded in 2 large human immunodeficiency virus (HIV) observational studies from North America, approximately half were classified as type 2. In the REPRIEVE clinical trial of pitavastatin versus placebo in people with HIV (PWH) (<3% of participants were from Europe), 20.6% of MIs were type 2. The proportions of type 1 MI (T1MI) and type 2 MI (T2MI) in European PWH are unknown.
Methods: The study included a retrospective record review, ascertainment of prospectively recorded and medically validated MIs, differentiation of T1MI and T2MI, and MI time trend analysis in the Swiss HIV Cohort Study (1 January 2000 to 31 May 2021). Exploratory analysis was performed of the associations of T1MI and T2MI with blood leukocyte count and 2 validated genome-wide coronary artery disease-associated polygenic risk scores (metaGRS and GPSmult).
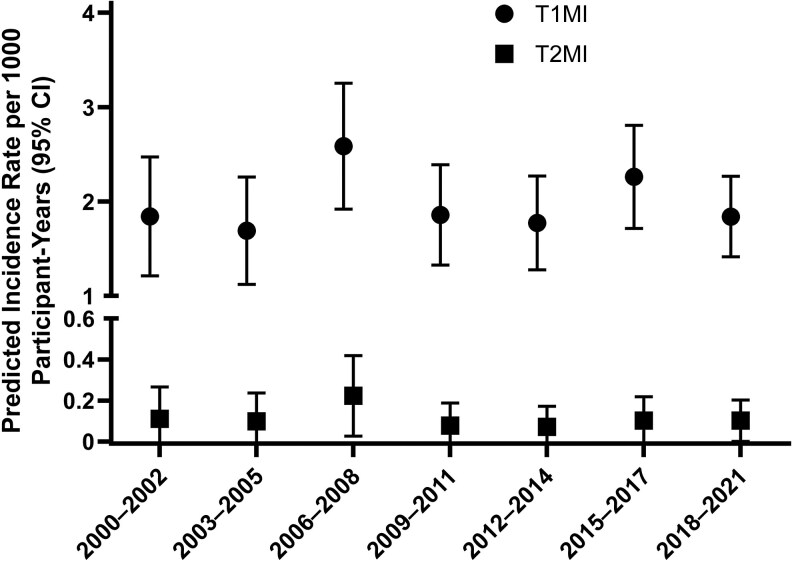
Results: Between 2000 and 2021, 16 027 Swiss HIV Cohort Study participants accumulated 181 598 years of follow-up, and 379 had a validated first MI. Of these participants, 359 (94.7%) had T1MI, and 20 (5.3%) had T2MI. Invasive coronary angiography was done in 95% and 60% of participants with T1MI and T2MI, respectively. We found no evidence for increasing or decreasing incidence trends over time for T1MI (P = .86) or T2MI (P = .85). Participants in the highest quintile for leukocyte count, metaGRS, and GPSmult had significantly increased adjusted odds ratios for T1MI; power was limited for detecting associations with T2MI.
Conclusions: The proportion of T2MI in PWH in Switzerland is approximately 5%, consistent with data from the general population and lower than in previous North American reports among PWH.
Keywords: HIV infection; myocardial infarction; time trends; type 1 myocardial infarction; type 2 myocardial infarction.
© The Author(s) 2025. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. D. L. B. has received honoraria for advisory boards from Gilead, ViiV, and MSD. C. R. K. reports grants/support from Gilead, paid to their institution, outside the submitted work. E. B. has received consulting fees from Gilead, MSD, ViiV, Pfizer, and AbbVie and travel support from Gilead, MSD, and Pfizer, all paid to their institution and all outside the submitted work. M. C. reports grants/support and payment for expert testimony from Gilead, MSD, and ViiV and travel support from Gilead, all paid to their institution and all outside the submitted work. H. F. G., outside this study and all outside the submitted work, reports grants from Gilead (unrestricted research grant) and the Yvonne Jacob Foundation, paid to their institution; personal fees as an advisor/consultant for Merck, ViiV, Johnson & Johnson, GSK, Janssen, Novartis, and Gilead; and data and safety monitoring board remuneration from Merck. B. L. received personal fees from Kantonsspital Baselland Liestal, Switzerland (for consultancy and statistical analyses), during the conduct of the study, and reports personal fees from Gilead for lectures and ViiV for advisory board service, outside the submitted work. P. E. T.'s institution reports unrestricted and educational grants from Gilead, ViiV, and MSD, and advisory fees from Gilead and ViiV, all outside the submitted work. All other authors report no potential conflicts.
Figures


References
-
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J 2019; 40:237–69. - PubMed
