

Standard and accelerated crosslinking protocols in keratoconus - differences and evolution at one year
- PMID: 40698114
- PMCID: PMC12277981
- DOI: 10.22336/rjo.2025.29
Standard and accelerated crosslinking protocols in keratoconus - differences and evolution at one year
Abstract
Objectives: Keratoconus (KC) is a bilateral, progressive corneal ectasia that involves corneal thinning and a decrease in visual acuity. Stopping the progression of keratoconus can be achieved through various photooxidative crosslinking (CXL) methods. The objective of this study was to compare two protocols of epi-off corneal crosslinking-the standard and the accelerated protocol-in terms of efficacy after a one-year follow-up.
Methods: 41 eyes with progressive keratoconus were treated with corneal crosslinking, either using the accelerated (Acc-CXL) or standard protocol (Std-CXL). The following parameters were monitored: refraction, corneal diopter power on topographic maps (Kmax and Kmin), corneal thickness (CCT), resistance factor (CRF), hysteresis, and the depth of the demarcation line. All measurements were repeated 12 months after the intervention.
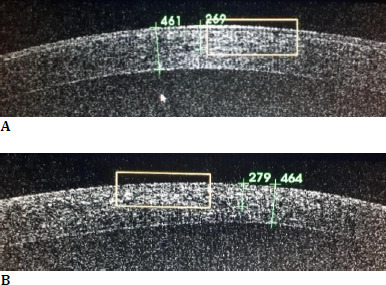
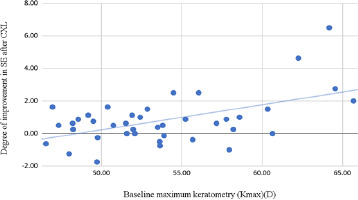
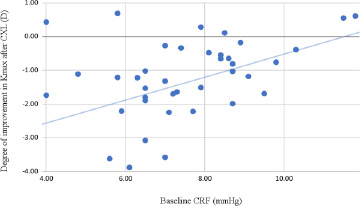
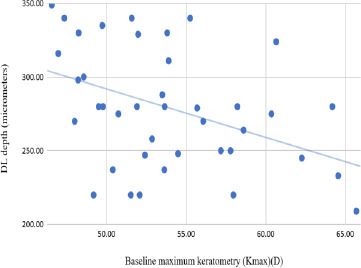
Results: The progression of keratoconus was halted in 20 eyes using the accelerated method and in 21 eyes using the standard procedure. Both methods resulted in a statistically significant regression of the spherical equivalent, Kmax, and an increase in CCT and CRF, without substantial differences in efficacy. The demarcation line was highlighted on average at a depth of 278.9 ± 31.71 micrometres for the Acc-CXL group and 280.42 ± 47.85 micrometres for the Std-CXL group. It was correlated with the initial topographical values.
Discussion: The evaluation of patients revealed no progression of keratoconus following the procedure. Approximately 40% of the cases in the accelerated protocol group and 38.09% of the cases in the standard protocol group have maintained the parameters at a constant level. In comparison, approximately 60% of the cases have shown improvements. An Australian registry revealed that both CXL protocols are safe and effective; however, the standard procedure leads to improved visual acuity, a more significant flattening of the steepest meridian, and a higher chance of an effect greater than one diopter power.
Conclusions: Corneal crosslinking (CXL) was effective in halting the progression of keratoconus using both methods. Accelerated CXL is faster and more comfortable for patients, with similar efficiency to standard CXL.
Keywords: CH = Corneal hysteresis; CRF = Corneal resistance factor; CXL = Corneal collagen crosslinking; IOPcc = Cornea-correlated IOP; IOPg = Goldmann-correlated intraocular pressure; KC = Keratoconus; accelerated protocol; corneal biomechanics; corneal crosslinking; keratoconus; standard protocol.
© 2025 The Authors.
Conflict of interest statement
The authors state no conflict of interest.
Figures
References
-
- Burcel MG, Corbu C, Coviltir V, Potop V, Constantin M, Dascalescu D, et al. Corneal crosslinking in progressive keratoconus: Comparison of dextran-based and hydroxypropyl methylcellulose-based riboflavin solutions-differences in demarcation line depth and 1 year outcomes. Rev Chim. 2019;70(4):1152–6.
-
- Ghaffari R, Hashemi H, Asghari S. IntechOpen. 2019. Intraoperative OCT for Monitoring Corneal Pachymetry during Corneal Collagen Cross-Linking for Keratoconus. In: A Practical Guide to Clinical Application of OCT in Ophthalmology. - DOI
-
- Hashemi H, Heydarian S, Hooshmand E, Saatchi M, Yekta A, Aghamirsalim M, et al. The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis. Cornea [Internet] 2020 Feb; [cited 2025 Apr 21];39(2) https://pubmed.ncbi.nlm.nih.gov/31498247/ - PubMed
-
- Huang AJ, Tseng SC, Kenyon KR. Paracellular permeability of corneal and conjunctival epithelia. Investigative ophthalmology & visual science [Internet] 1989 Apr; [cited 2025 Apr 21];30(4). doi: https://pubmed.ncbi.nlm.nih.gov/2703309/ - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials