

An Atypical Case of Infectious Myositis in a Young Woman on Immunosuppressive Therapy
- PMID: 40698230
- PMCID: PMC12282974
- DOI: 10.7759/cureus.86545
An Atypical Case of Infectious Myositis in a Young Woman on Immunosuppressive Therapy
Abstract
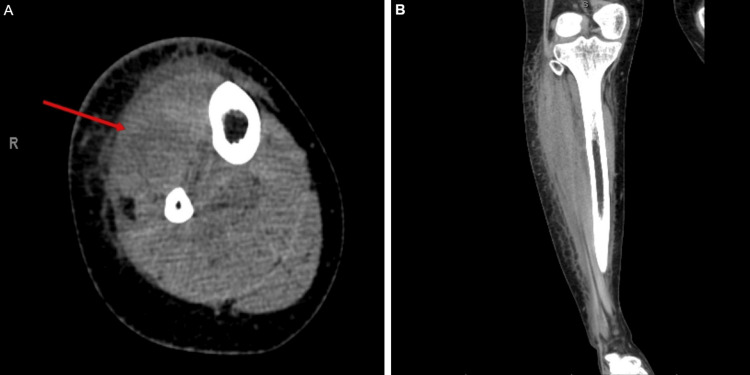
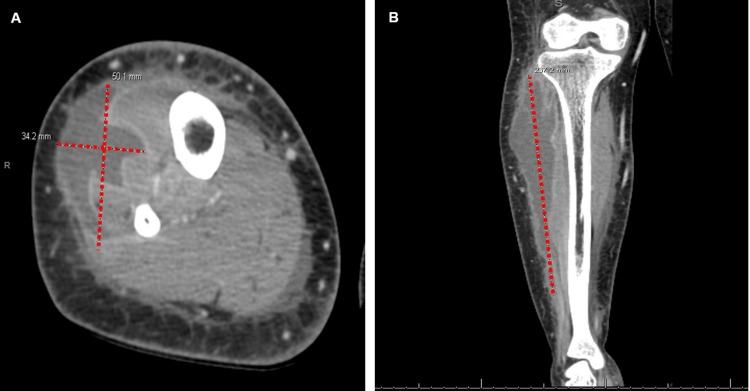
Infectious myositis is a rare but serious condition typically caused by bacterial pathogens. In immunocompromised patients, including those on long-term immunosuppressive therapy, clinical signs of myositis can be subtle or delayed. We present the case of a 21-year-old woman with systemic lupus erythematosus (SLE) on immunosuppressive therapy who presented with pain, fever, tachycardia, and swelling of the right lower leg. Initial evaluation revealed no skin defects or rash and normal creatine phosphokinase (CPK) levels. A non-contrast computed tomography (CT) scan of her leg showed some soft tissue changes, but it was only after a week of worsening symptoms that contrast-enhanced CT imaging revealed a multiloculated, large abscess, measuring 23.7 cm in length, in the anterior compartment of the leg. The abscess was drained surgically, and intraoperative cultures grew methicillin-resistant Staphylococcus aureus. The absence of early definitive findings, including a normal CPK level, may have contributed to the delay in diagnosis. This case highlights the diagnostic challenges of infectious myositis in immunosuppressed patients, where early imaging and laboratory findings can be misleading, underscoring the importance of repeated clinical assessment and timely advanced imaging to ensure early detection and appropriate treatment.
Keywords: acute myositis; bacterial myositis; bacterial pyomyositis; infectious myositis; pyomyositis; soft tissue infection.
Copyright © 2025, Abad et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Purulent infectious myositis (formerly tropical pyomyositis) Habeych ME, Trinh T, Crum-Cianflone NF. J Neurol Sci. 2020;413:116767. - PubMed
-
- Necrotizing myositis: highlighting the hidden depths - case series and review of the literature. Khanna A, Gurusinghe D, Taylor D. ANZ J Surg. 2020;90:130–134. - PubMed
-
- Imaging of musculoskeletal soft tissue infections. Turecki MB, Taljanovic MS, Stubbs AY, Graham AR, Holden DA, Hunter TB, Rogers LF. Skeletal Radiol. 2010;39:957–971. - PubMed
-
- Infective pyomyositis and myositis in children in the era of community-acquired, methicillin-resistant Staphylococcus aureus infection. Pannaraj PS, Hulten KG, Gonzalez BE, Mason EO Jr, Kaplan SL. Clin Infect Dis. 2006;43:953–960. - PubMed
Publication types
LinkOut - more resources
Full Text Sources