

Smoking, Colchicine and Postoperative Outcomes in Thoracic Surgery: Post Hoc Analysis of the COP-AF Randomized Controlled Trial
- PMID: 40698308
- PMCID: PMC12277807
- DOI: 10.1016/j.cjco.2025.04.008
Smoking, Colchicine and Postoperative Outcomes in Thoracic Surgery: Post Hoc Analysis of the COP-AF Randomized Controlled Trial
Abstract
Background: To determine, among patients who underwent major noncardiac thoracic surgery, the association between smoking and perioperative atrial fibrillation (AF) and myocardial injury after noncardiac surgery (MINS), and whether the effect of colchicine use on these outcomes varied by smoking status.
Methods: This study is a subgroup analysis of the Colchicine for the Prevention of Perioperative Atrial Fibrillation (COP-AF) randomized clinical trial. A total of 3209 participants who underwent major noncardiac thoracic surgery were randomized to receive colchicine, 0.5 mg twice daily, or identical placebo, for 10 days starting 2-4 hours before surgery. The co-primary outcomes were clinically significant perioperative AF and MINS during the 14-day follow-up.
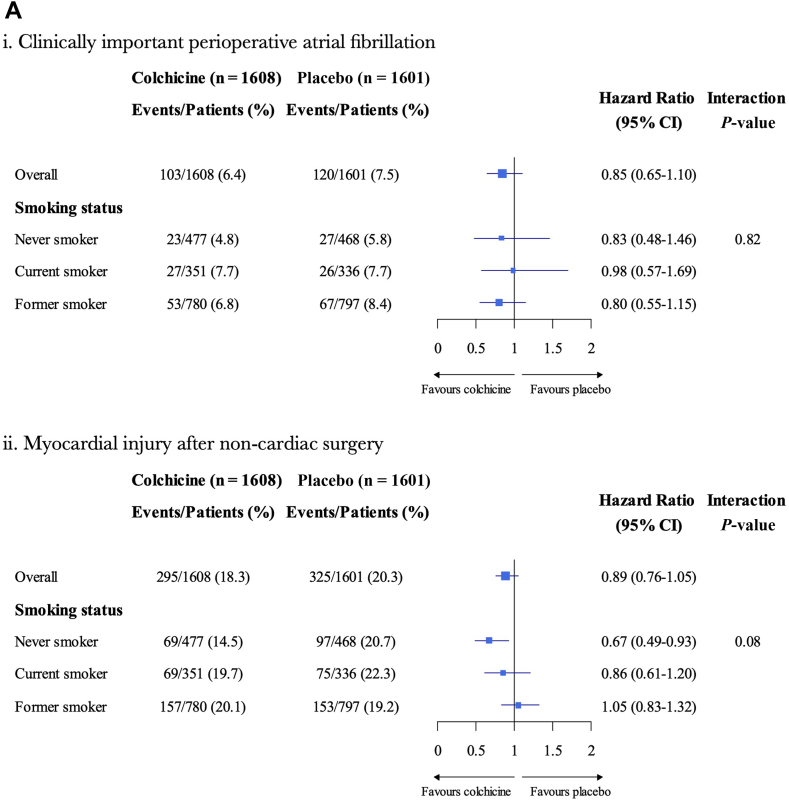
Results: A total of 687 (21.4%) were current smokers, 1577 (49.1%) were former smokers, and 945 (29.5%) were never smokers. AF occurred in 7.7%, 7.6%, and 5.3%, and MINS occurred in 21.0%, 19.7%, and 17.6% of current, former, and never smokers, respectively. Compared to never smokers, the adjusted hazard ratio for AF was 1.72 (95% confidence interval [CI] 1.07-2.77, P = 0.02) in current smokers and 1.46 (95% CI 0.99-2.16, P = 0.06) in former smokers, and the adjusted hazard ratio for MINS was 1.16 (95% CI 0.87-1.54, P = 0.32) in current smokers and 1.02 (95% CI 0.81-1.28, P = 0.88) in former smokers. No interaction occurred between smoking status and colchicine allocation for AF (interaction P, 0.82) or MINS (interaction P, 0.08).
Conclusions: Current smoking was associated with a small but increased risk of perioperative AF but not MINS after thoracic surgery. The effect of colchicine use on either outcome was not modified by smoking status.
Clinical trial registration: NCT03310125.
Contexte: Déterminer le lien entre le tabagisme, la fibrillation auriculaire (FA) periopératoire et les lésions myocardiques après une chirurgie non cardiaque chez des patients ayant subi une chirurgie thoracique majeure non cardiaque, et établir si l’effet de la colchicine sur ces paramètres varie en fonction du statut tabagique.
Méthodologie: Il s’agit d’une analyse de sous-groupes de l’essai clinique COP-AF (Colchicine for the Prevention of Perioperative Atrial Fibrillation) dans le cadre de laquelle 3 209 participants ayant subi une chirurgie thoracique majeure non cardiaque ont été répartis aléatoirement pour recevoir de la colchicine à raison de 0,5 mg deux fois par jour ou un placebo identique pendant 10 jours, à compter de 2 à 4 heures avant l’intervention chirurgicale. Les paramètres d’évaluation principaux conjoints étaient une FA périopératoire et les lésions myocardiques cliniquement significatives pendant un suivi de 14 jours.
Résultats: Au total, 687 participants (21,4 %) étaient fumeurs; 1 577 (49,1 %) étaient des ex-fumeurs et 945 (29,5 %) n’avaient jamais fumé. Une FA a été observée chez 7,7 %, 7,6 % et 5,3 %, et des lésions myocardiques chez 21,0 %, 19,7 % et 17,6 % des fumeurs, des ex-fumeurs et des participants n’ayant jamais fumé, respectivement. Comparativement aux participants n’ayant jamais fumé, le rapport de risques ajusté (RRA) pour la FA a été de 1,72 (intervalle de confiance [IC] à 95 % : 1,07-2,77; p = 0,02) chez les fumeurs et de 1,46 (IC à 95 % : 0,99-2,16; p = 0,06) chez les ex-fumeurs, et le RRA pour les lésions myocardiques, de 1,16 chez les fumeurs (IC à 95 % : 0,87-1,54; p = 0,32) et de 1,02 chez les ex-fumeurs (IC à 95 % : 0,81-1,28; p = 0,88). Aucune interaction n’a été observée entre le statut tabagique et l’affectation au groupe traité par la colchicine pour une FA (valeur p de l’interaction = 0,82) ou une lésion myocardique (valeur p de l’interaction = 0,08).
Conclusion: Chez les fumeurs, le risque de FA périopératoire était légèrement plus élevé, ce qui n’était pas le cas pour les lésions myocardiques après une chirurgie thoracique. L’effet de la colchicine sur l’un ou l’autre de ces paramètres n’a pas été modifié par le statut tabagique.
Enregistrement de l’essai clinique: ClinicalTrials.gov, NCT03310125.
© 2025 The Authors.
Figures



References
-
- Moller A.M., Villebro N., Pedersen T., Tonnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002;359:114–117. - PubMed
-
- Grønkjær M., Eliasen M., Skov-Ettrup L.S., et al. Preoperative smoking status and postoperative complications: a systematic review and meta-analysis. Ann Surg. 2014;259:52–71. - PubMed
-
- Yamamichi T., Ichinose J., Iwamoto N., et al. Correlation between smoking status and short-term outcome of thoracoscopic surgery for lung cancer. Ann Thorac Surg. 2022;113:459–465. - PubMed
-
- King M., Howell G., Hunter V. Hospital readmission rates within 30 days following thoracic oncology surgery. J Thorac Oncol. 2017;12(1 Suppl 1):S1108–S1109.
-
- Mason D.P., Subramanian S., Nowicki E.R., et al. Impact of smoking cessation before resection of lung cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database study. Ann Thorac Surg. 2009;88:362–371. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
