

Association between the Venous Excess Ultrasound (VExUS) score and acute kidney injury in critically ill patients with sepsis: a multicenter prospective observational study
- PMID: 40699273
- PMCID: PMC12287484
- DOI: 10.1186/s13613-025-01529-w
Association between the Venous Excess Ultrasound (VExUS) score and acute kidney injury in critically ill patients with sepsis: a multicenter prospective observational study
Abstract
Background: Venous congestion is associated with adverse clinical outcomes in critically ill patients, yet its assessment remains challenging. Recently, the Venous Excess Ultrasound (VExUS) score has shown great potential as a non-invasive tool for assessing venous congestion in cardiac patients. However, the relationship between VExUS and clinical outcomes in patients with sepsis remains understudied. This study aims to evaluate the incidence of venous congestion based on VExUS assessment within the first 5 days of intensive care unit (ICU) admission in critically ill patients with sepsis, and to investigate the association between VExUS and clinical outcomes.
Methods: We conducted a prospective, observational study in four ICUs, enrolling adult patients with sepsis who stayed in the ICU for at least 24 h. VExUS assessments were performed on days 1 (within 24 h), 3 (48-72 h), and 5 (96-120 h) following ICU admission. Patients were classified according to VExUS score ≥ 2 or < 2. The primary outcome was the prevalence of acute kidney injury (AKI) during ICU stay, while secondary outcomes included 30-day mortality, ICU mortality, and requirement for renal replacement therapy (RRT).
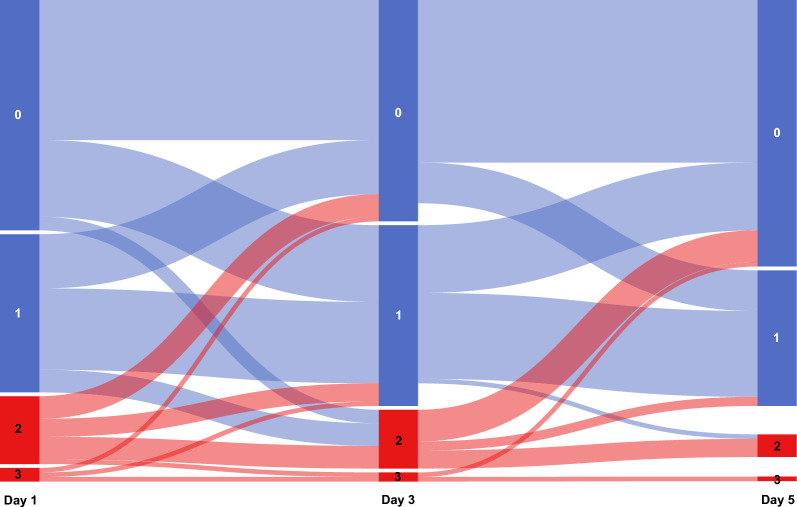
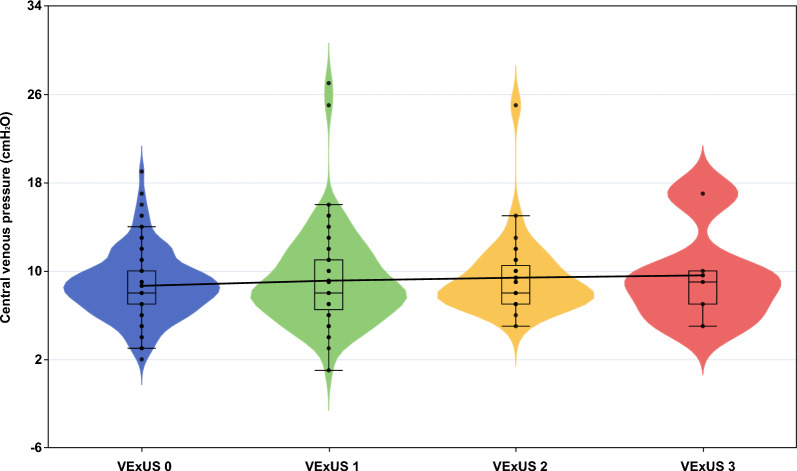
Results: Among the 108 patients included, 18% (19 patients) showed VExUS score ≥ 2 on day 1 of ICU admission, and the prevalence progressively decreased to 15% (15 patients) by day 3 and 6% (6 patients) by day 5. The VExUS score ≥ 2 was not associated with AKI (OR 1.82, 95% CI 0.62-5.31, p = 0.274), 30-day mortality (OR 0.82, 95% CI 0.28-2.4, p = 0.711), ICU mortality (OR 1.12, 95% CI 0.41-3.04, p = 0.82), or requirement for RRT (OR 2.29, 95% CI 0.68-7.64, p = 0.179). There was no significant correlation between VExUS and central venous pressure (coefficient: - 0.019, 95% CI -0.01 to 0.05, p = 0.204).
Conclusion: In critically ill patients with sepsis, approximately 20% exhibit early (within 24 h of ICU admission) venous congestion, with the prevalence progressively decreasing over the subsequent 5 days. Venous congestion assessed by VExUS was not associated with the occurrence of AKI or with mortality.
Trial registration: Chinese Clinical Trial Registry, ChiCTR2200066987. Registered 22 December 2022, https://www.chictr.org.cn/.
Keywords: Acute kidney injury; ICU; Mortality; Sepsis; Ultrasound; VExUS; Venous congestion.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by an independent ethics committee (protocol number: 2022-124K). All participants provided written informed consent to participate. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
EARLY TRAJECTORY OF VENOUS EXCESS ULTRASOUND SCORE IS ASSOCIATED WITH CLINICAL OUTCOMES OF GENERAL ICU PATIENTS.Shock. 2024 Mar 1;61(3):400-405. doi: 10.1097/SHK.0000000000002321. Epub 2024 Feb 27. Shock. 2024. PMID: 38517247
-
Relationship Between Cumulative Fluid Balance and the Degree of Venous Congestion According to VExUS Score in Critically Ill Patients in a General Intensive Care Unit.J Ultrasound Med. 2025 Sep;44(9):1545-1554. doi: 10.1002/jum.16709. Epub 2025 May 16. J Ultrasound Med. 2025. PMID: 40377372
-
Coexistence of a fluid responsive state and venous congestion signals in critically ill patients: a multicenter observational proof-of-concept study.Crit Care. 2024 Feb 19;28(1):52. doi: 10.1186/s13054-024-04834-1. Crit Care. 2024. PMID: 38374167 Free PMC article.
-
Intensity of continuous renal replacement therapy for acute kidney injury.Cochrane Database Syst Rev. 2016 Oct 4;10(10):CD010613. doi: 10.1002/14651858.CD010613.pub2. Cochrane Database Syst Rev. 2016. PMID: 27699760 Free PMC article.
-
Automated monitoring compared to standard care for the early detection of sepsis in critically ill patients.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD012404. doi: 10.1002/14651858.CD012404.pub2. Cochrane Database Syst Rev. 2018. PMID: 29938790 Free PMC article.
References
-
- Meyer NJ, Prescott HC. Sepsis and septic shock. N Engl J Med. 2024;391:2133–46. - PubMed
-
- Zampieri FG, Bagshaw SM, Semler MW. Fluid therapy for critically ill adults with sepsis: a review. JAMA. 2023;329:1967. - PubMed
-
- Sakr Y, Rubatto Birri PN, Kotfis K, Nanchal R, Shah B, Kluge S, et al. Higher fluid balance increases the risk of death from sepsis: results from a large international audit. Crit Care Med. 2017;45:386–94. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
