

Sympathetic Responses to Antihypertensive Treatment Strategies : Implications for the Residual Cardiovascular Risk
- PMID: 40699460
- PMCID: PMC12287247
- DOI: 10.1007/s11906-025-01339-2
Sympathetic Responses to Antihypertensive Treatment Strategies : Implications for the Residual Cardiovascular Risk
Abstract
Purpose of Review: To examine whether and to what extent lifestyle, pharmacological and device-based therapeutic blood pressure lowering interventions are capable to restore a normal sympathetic cardiovascular function in hypertensive patients.
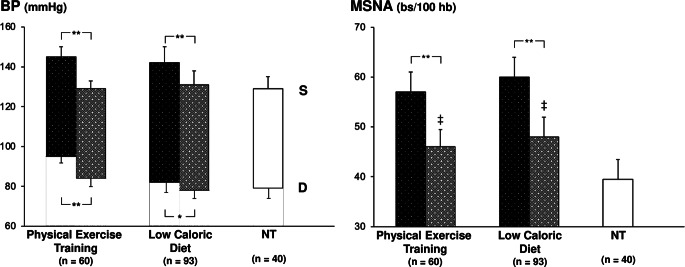
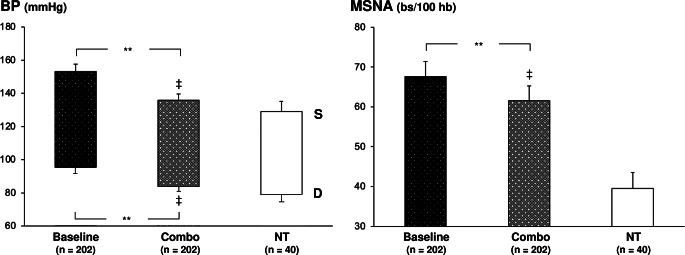
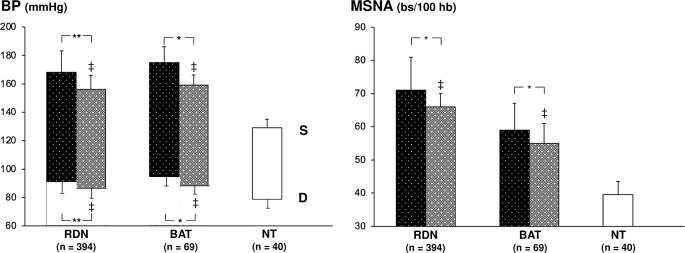
Recent Findings: Data collected by examining the results of more than 50 studies published during the past years by directly quantifying, via microneurography, the sympathetic nerve traffic responses to non-pharmacological and pharmacological antihypertensive treatment have shown that no normalization of the sympathetic cardiovascular function is achieved. Recently, a study by our group carried out in 219 hypertensive patients under monotherapy or combination drug treatment confirmed these results, by showing that, despite achieving an optimal blood pressure control, antihypertensive treatment fails to restore the normal sympathetic neural function detected in the normotensive healthy subjects.
Summary: The sympathetic nervous system plays a key role in blood pressure regulation and hypertension pathophysiology. Recent findings document its involvement also in determining the blood pressure lowering effects of antihypertensive agents. However, the available data show the inability to achieve during treatment a full sympathetic normalization, a finding which may represent one of the mechanisms responsible for the residual cardiovascular risk of the treated hypertensive patient.
Keywords: Antihypertensive drug treatment; Carotid baroreceptor stimulation; Lifestyle interventions; Muscle sympathetic nerve traffic; Renal denervation; Residual cardiovascular risk; Sympathetic activity.
Conflict of interest statement
Declarations. Ethical Approval: Human and Animal Rights and Informed Consent. All reported studies/ experiments with human subjects or animals performed by the authors have been previously published and complied with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/ national/ institutional guidelines. Competing Interests: The authors declare no competing interests.
Figures


Similar articles
-
Renal denervation for resistant hypertension.Cochrane Database Syst Rev. 2017 Feb 21;2(2):CD011499. doi: 10.1002/14651858.CD011499.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2021 Nov 22;11:CD011499. doi: 10.1002/14651858.CD011499.pub3. PMID: 28220472 Free PMC article. Updated.
-
Renal denervation for resistant hypertension.Cochrane Database Syst Rev. 2021 Nov 22;11(11):CD011499. doi: 10.1002/14651858.CD011499.pub3. Cochrane Database Syst Rev. 2021. PMID: 34806762 Free PMC article.
-
Dynamic analysis of renal nerve activity responses to baroreceptor denervation in hypertensive rats.Hypertension. 2001 Apr;37(4):1153-63. doi: 10.1161/01.hyp.37.4.1153. Hypertension. 2001. PMID: 11304518
-
Central action of alpha-adrenoceptor agents on the baroreceptor reflex.J Auton Nerv Syst. 1992 Nov;41(1-2):93-101. doi: 10.1016/0165-1838(92)90131-y. J Auton Nerv Syst. 1992. PMID: 1362732
-
Sympathetic Vasomotion Reflects Catheter-Based Radiofrequency Renal Denervation.Hypertension. 2025 Jul;82(7):1261-1270. doi: 10.1161/HYPERTENSIONAHA.125.24980. Epub 2025 May 27. Hypertension. 2025. PMID: 40421540
References
-
- Esler MD, Osborn JW, Schlaich MP. Sympathetic pathophysiology in hypertension origins: the path to renal denervation. Hypertension. 2024;81:1194–205. - PubMed
-
- Noll G, Wenzel RR, Schneider M, Oesch V, Binggeli C, Shaw S, et al. Increased activation of sympathetic nervous system and endothelin by mental stress in normotensive offspring of hypertensive parents. Circulation. 1996;93:866–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
