

Contrast enhanced ultrasound - a useful method for diagnosing tubal ectopic pregnancy with low level β-HCG
- PMID: 40699483
- PMCID: PMC12287497
- DOI: 10.1186/s13089-025-00438-0
Contrast enhanced ultrasound - a useful method for diagnosing tubal ectopic pregnancy with low level β-HCG
Abstract
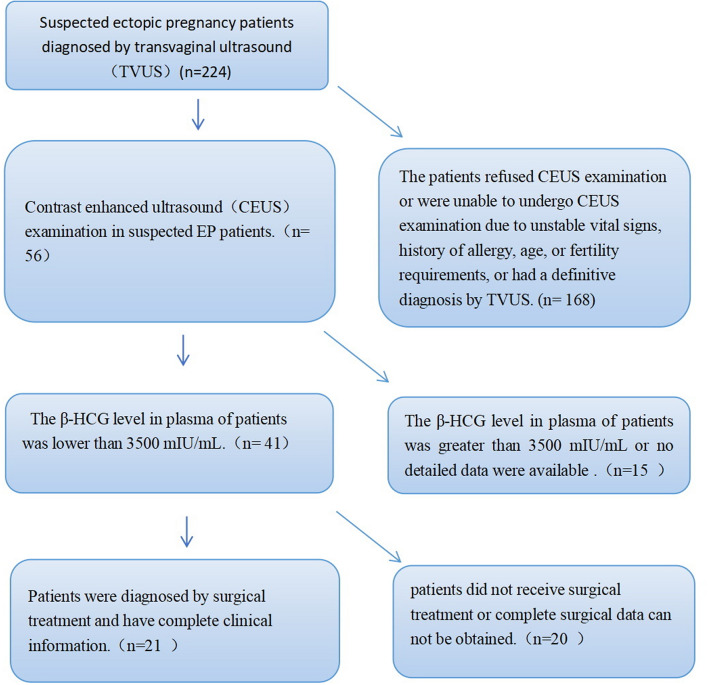
Background: In patients presenting with atypical symptoms or low plasma β-HCG levels, the presence of an adnexal mass without a yolk sac or embryo on ultrasound often provides insufficient confidence for a definitive diagnosis of ectopic pregnancy(EP). Consequently, most such cases can only be classified as suspected EP. This study aimed to evaluate the diagnostic value of contrast enhanced ultrasound (CEUS) for tubal EP (tEP). We retrospectively analyzed 21 patients with suspected EP who underwent CEUS between August 2017 and August 2024. All patients had plasma β-HCG levels below 3500 mIU/mL. Among them, 20 underwent laparoscopic surgery, and all underwent curettage. The diagnostic performance of CEUS for tEP was assessed.
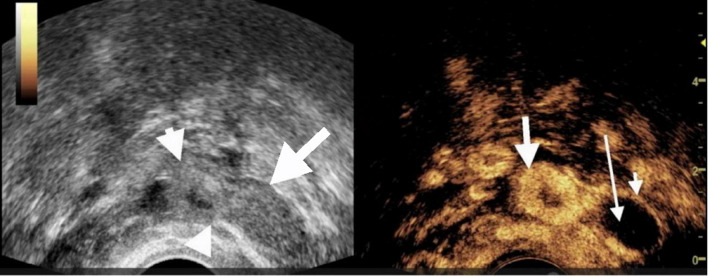
Results: A total of 21 patients were included: 19 with tEP, 1 with ovarian pregnancy, and 1 with intrauterine pregnancy. The sensitivity, specificity, and accuracy of transvaginal ultrasound (TVUS) for diagnosing tubal dilation were 15.8%, 100%, and 23.8%, respectively. For CEUS, these values were 94.7%, 100%, and 95.2%, respectively. Statistically significant differences were observed between CEUS and TVUS in sensitivity and accuracy (P = 0.000). The enhancement pattern of villous tissue was categorized as either circular or non-circular. Among the tEP cases, 2 exhibited circular enhancement and 17 showed non-circular enhancement. Based on positive β-HCG, absence of an intrauterine gestational sac, and sonographic visualization of a dilated fallopian tube containing either circular or non-circular enhancement internally, CEUS demonstrated high diagnostic accuracy for tEP diagnosis in cases with low β-HCG levels. CEUS correctly diagnosed 18 of 19 tEP cases. One tEP case was diagnosed as a mass of uncertain significance. The intrauterine pregnancy case was misdiagnosed as an EP. The ovarian pregnancy case was diagnosed as EP, though CEUS indicated a relatively high possibility of ovarian origin.
Conclusion: In conclusion, CEUS holds significant diagnostic value for tEP. It is particularly useful in diagnostically unclear cases and provides a more detailed assessment of the internal structure of adnexal masses.
Keywords: Contrast media; Ectopic; Fallopian tubes; Pregnancy; Ultrasonography.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the ethics committee of Dongzhimen Hospital of Beijing University of Chinese Medicine(2024DZMEC-665-02).The study adhered to the principles outlined in the Helsinki Declaration of 1975, as revised in 2013. Consent for publication: Not applicable. Competing interests: The authors have no conflicts of interest to disclose.
Figures




Similar articles
-
Contrast-enhanced ultrasound for the diagnosis of hepatocellular carcinoma in adults with chronic liver disease.Cochrane Database Syst Rev. 2022 Sep 2;9(9):CD013483. doi: 10.1002/14651858.CD013483.pub2. Cochrane Database Syst Rev. 2022. PMID: 36053210 Free PMC article.
-
Contrast-enhanced ultrasound using SonoVue® (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2013 Apr;17(16):1-243. doi: 10.3310/hta17160. Health Technol Assess. 2013. PMID: 23611316 Free PMC article.
-
Intraoperative frozen section analysis for the diagnosis of early stage ovarian cancer in suspicious pelvic masses.Cochrane Database Syst Rev. 2016 Mar 1;3(3):CD010360. doi: 10.1002/14651858.CD010360.pub2. Cochrane Database Syst Rev. 2016. PMID: 26930463 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
First trimester ultrasound tests alone or in combination with first trimester serum tests for Down's syndrome screening.Cochrane Database Syst Rev. 2017 Mar 15;3(3):CD012600. doi: 10.1002/14651858.CD012600. Cochrane Database Syst Rev. 2017. PMID: 28295158 Free PMC article.
References
-
- Centers for Disease Control and Prevention (CDC) (1995) Ectopic pregnancy–United states, 1990–1992. MMWR Morb Mortal Wkly Rep 44:46–48 - PubMed
-
- Rouse CE, Eckert LO, Babarinsa I et al (2017) Global alignment of immunization safety in pregnancy (GAIA) abortion work group; Brighton collaboration abortion working group. Spontaneous abortion and ectopic pregnancy: case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data, vol 35. Vaccine, pp 6563–6574 - PMC - PubMed
-
- Creanga AA, Shapiro-Mendoza CK, Bish CL, Zane S, Berg CJ, Callaghan WM (2011) Trends in ectopic pregnancy mortality in the united states: 1980–2007. Obstet Gynecol 117:837–843 - PubMed
-
- Berg CJ, Callaghan WM, Syverson C, Henderson Z (2010) Pregnancy-related mortality in the united states, 1998 to 2005. Obstet Gynecol 116:1302–1309 - PubMed
LinkOut - more resources
Full Text Sources