

Response to corticosteroids and alternative therapies in sarcoidosis-related hypercalcemia: A guideline-lacking retrospective analysis
- PMID: 40699493
- PMCID: PMC12242867
- DOI: 10.36141/svdld.v42i2.16239
Response to corticosteroids and alternative therapies in sarcoidosis-related hypercalcemia: A guideline-lacking retrospective analysis
Abstract
Background and aim: Sarcoidosis is a systemic inflammatory disease of unknown etiology that can affect multiple organs including a known complication of hypercalcemia. Many therapies, both steroidal and nonsteroidal, have been employed. However, the optimal therapy for hypercalcemia in sarcoidosis is unknown, with most data from case reports and small case series. More information is needed to determine which nonsteroidal agents control hypercalcemia in sarcoidosis patients, particularly for populations in whom steroids should be avoided. We sought to answer the question, which pharmacological agents control hypercalcemia in patients diagnosed with sarcoidosis?
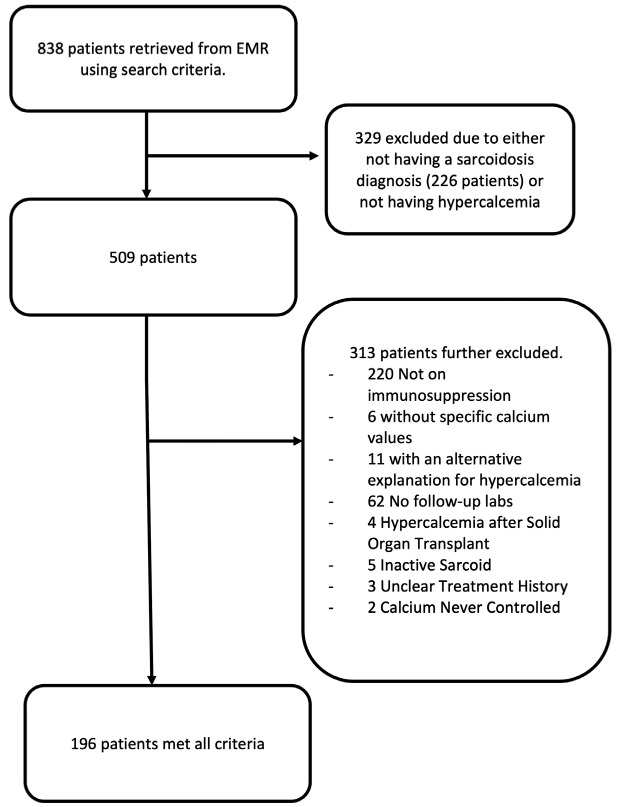
Methods: We performed a retrospective chart review on all adult patients at our hospital a diagnosis of Sarcoidosis and Hypercalcemia and a recorded calcium level of greater than 10.4 mg/dL. We then determined which agents were able to control their calcium to a level of 10.4 mg/dL or less for at least 6 months and 12 months.
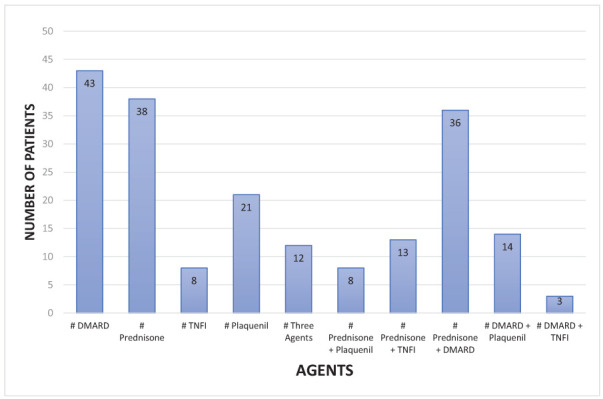
Results: The most common efficacious treatments were prednisone, methotrexate, hydroxychloroquine, and prednisone + methotrexate. A positive linear relationship was found between ACE and highest calcium levels. No significant relationship between organ involvement or race and highest calcium levels were noted.
Conclusions: There is currently little data or guidelines to best guide the treatment of hypercalcemia in sarcoidosis. This study represents the first with the primary aim to compare treatment options for hypercalcemia in sarcoidosis across a large cohort. Several non-steroidal options were identified that controlled hypercalcemia as a single agent. In addition, this study further investigated potential biomarkers for abnormal calcium metabolism as well as the relationship between calcium levels and organ involvement/race. Further work is needed to determine the most effective steroid sparing therapy to control hypercalcemia in sarcoidosis.
Conflict of interest statement
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article.
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 9;1(1):CD011535. doi: 10.1002/14651858.CD011535.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Apr 19;4:CD011535. doi: 10.1002/14651858.CD011535.pub4. PMID: 31917873 Free PMC article. Updated.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
References
-
- Baughman RP, Janovcik J, Ray M, Sweiss N, Lower EE. Calcium and vitamin D metabolism in sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. 2013;30(2):113–20. - PubMed
-
- Sharma OP. Vitamin D, calcium, and sarcoidosis. Chest. 1996;109(2):535–9. doi: 10.1378/chest.109.2.535. - PubMed
-
- Baughman RP, Teirstein AS, Judson MA, et al. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001;164(10 Pt 1):1885–9. doi: 10.1164/ajrccm.164.10.2104046. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous