

The Role of Centralized Sexual Assault Care Centers in HIV Post-Exposure Prophylaxis Treatment Adherence: A Retrospective Single Center Analysis
- PMID: 40700323
- PMCID: PMC12286241
- DOI: 10.3390/idr17040077
The Role of Centralized Sexual Assault Care Centers in HIV Post-Exposure Prophylaxis Treatment Adherence: A Retrospective Single Center Analysis
Abstract
Background: Sexual assault victims involving penetration are at risk of contracting human immunodeficiency virus (HIV). Post-exposure prophylaxis (PEP) can effectively prevent HIV infection if initiated promptly within 72 h following exposure and adhered to for 28 days. Nonetheless, therapeutic adherence amongst sexual assault victims is low. Victim-centered care, provided by specially trained forensic nurses and midwives, may increase adherence.
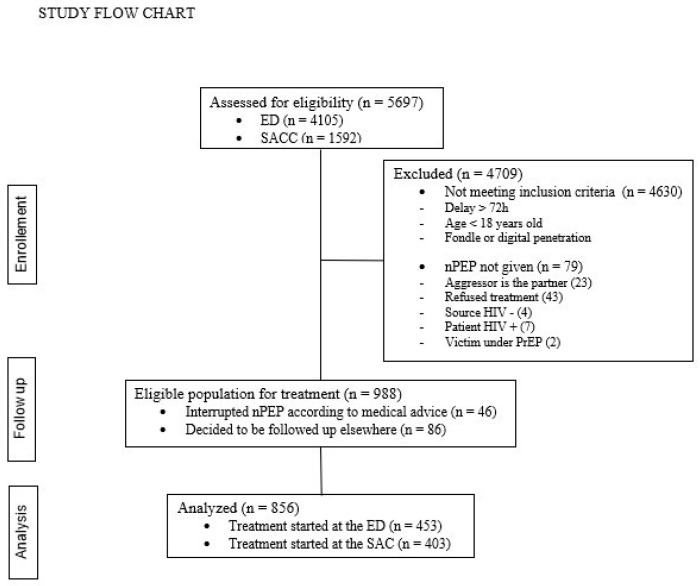
Methods: We conducted a retrospective case-control study to evaluate the impact of sexual assault center (SAC)-centered care on adherence to PEP compared to care received in the emergency department (ED). Data from January 2011 to February 2022 were reviewed. Multivariable logistic regression analysis was employed to determine the association between centralized specific care for sexual assault victims and completion of the 28-day PEP regimen. The secondary outcome assessed was provision of psychological support within 5 days following the assault.
Results: We analyzed 856 patients of whom 403 (47.1%) received care at a specialized center for sexual assault victims. Attendance at the SAC, relative to the ED, was not associated with greater probability of PEP completion both in the unadjusted (52% vs. 50.6%; odds ratio [OR]: 1.06, 95% CI: 0.81 to 1.39; p = 0.666) and adjusted (OR: 0.81, 95%CI 0.58-1.11; p = 0.193) analysis. The care provided at the SAC was associated with improved early (42.7% vs. 21.5%; p < 0.001) and delayed (67.3% vs. 33.7%; p < 0.001) psychological support.
Conclusions: SAC-centered care is not associated with an increase in PEP completion rates in sexual assault victims beyond the increase associated with improved access to early and delayed psychological support. Other measures to improve PEP completion rates should be developed. What is already known on this topic-Completion rates for HIV post-exposure prophylaxis (PEP) among victims of sexual assault are low. Specialized sexual assault centers, which provide comprehensive care and are distinct from emergency departments, have been suggested as a potential means of improving treatment adherence and completion rates. However, their actual impact on treatment completion remains unclear. What this study adds-This study found that HIV PEP completion rates in sexual assault victims were not significantly improved by centralized care in a specialized sexual assault center when compared to care initiated in the emergency department and continued within a sexually transmitted infection clinic. However, linkage to urgent psychological and psychiatric care was better in the specialized sexual assault center. How this study might affect research, practice or policy-Healthcare providers in sexual assault centers should be more aware of their critical role in promoting PEP adherence and improving completion rates. Policymakers should ensure that measures aimed at improving HIV PEP outcomes are implemented at all points of patient contact in these centers. Further research is needed to assess the cost-effectiveness of specialized sexual assault centers.
Keywords: non-occupational post-exposure prophylaxis; post-exposure prophylaxis; sexual assault; sexual assault victim; sexually transmitted diseases.
Conflict of interest statement
All the authors stated that they have no financial and personal relationships with other people or organizations that could inappropriately influence their work.
Figures
Similar articles
-
Antiretroviral post-exposure prophylaxis (PEP) for occupational HIV exposure.Cochrane Database Syst Rev. 2007 Jan 24;2007(1):CD002835. doi: 10.1002/14651858.CD002835.pub3. Cochrane Database Syst Rev. 2007. PMID: 17253483 Free PMC article.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
References
-
- Miele C., Maquigneau A., Joyal C.C., Bertsch I., Gangi O., Gonthier H., Rawlinson C., Vigourt-Oudart S., Symphorien E., Heasman A., et al. International guidelines for the prevention of sexual violence: A systematic review and perspective of WHO, UN Women, UNESCO, and UNICEF’s publications. Child Abus. Negl. 2023;146:106497. doi: 10.1016/j.chiabu.2023.106497. - DOI - PubMed
-
- Keygnaert I., De Schrijver L., Cismaru Inescu A., Schapansky E., Nobels A., Hahaut B., Stappers C., Debauw Z., Lemonne A., Renard B., et al. Understanding the Mechanism, Nature, Magnitude and Impact of Sexual Violence in Belgium. Belgian Science Policy; Brussels, Belgium: 2021. 117p (Final Report).
-
- Miller C.J., Li Q., Abel K., Kim E.-Y., Ma Z.-M., Wietgrefe S., La Franco-Scheuch L., Compton L., Duan L., Shore M.D., et al. Propagation and Dissemination of Infection after Vaginal Transmission of Simian Immunodeficiency Virus. J. Virol. 2005;79:9217–9227. doi: 10.1128/JVI.79.14.9217-9227.2005. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
