

Effects of CFTR Modulators on Pseudomonas aeruginosa Infections in Cystic Fibrosis
- PMID: 40700326
- PMCID: PMC12285981
- DOI: 10.3390/idr17040080
Effects of CFTR Modulators on Pseudomonas aeruginosa Infections in Cystic Fibrosis
Abstract
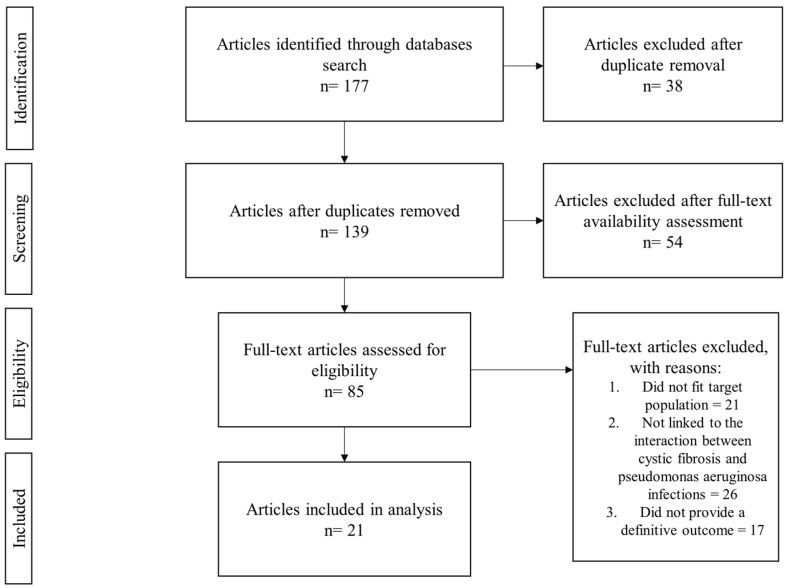
Background: Cystic fibrosis (CF) is an autosomal recessive disease caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. Modulator therapies have the ability to improve CFTR function in CF patients, but despite the clear evidence of benefits regarding CFTR modulator therapy, including improved lung function, the reduced rate of exacerbations, and an overall improved quality of life, studies focusing on the reduction rates of P. aeruginosa infections during modulator therapy expressed the need for future research on this topic. Objective: This study aimed to evaluate the impact of CFTR modulator therapies on the prevalence, density, and persistence of P. aeruginosa infection in CF patients and to explore the mechanisms involved. Methods: A systematic literature review was performed by searching five major databases (PubMed, Cochrane Library, Scopus, Google Scholar, and Web of Science), and 21 relevant articles investigating the link between CFTR therapy and P. aeruginosa infections were selected following the PRISMA guidelines. Results: The data indicated that Ivacaftor and the combination Elexacaftor/Tezacaftor/Ivacaftor (ETI) can reduce total bacterial load and markers of systemic inflammation. However, clonal lines of P. aeruginosa persist in most cases, and complete eradication is rare, mainly due to biofilm formation and antimicrobial resistance. Conclusions: Although CFTR-modulating therapies help to improve clinical condition and reduce inflammation, they do not consistently lead to the elimination of P. aeruginosa.
Keywords: Pseudomonas aeruginosa; biofilms; cystic fibrosis; lung infections; modulator therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Corrector therapies (with or without potentiators) for people with cystic fibrosis with class II CFTR gene variants (most commonly F508del).Cochrane Database Syst Rev. 2023 Nov 20;11(11):CD010966. doi: 10.1002/14651858.CD010966.pub4. Cochrane Database Syst Rev. 2023. PMID: 37983082 Free PMC article.
-
A grumbling concern: A survey of gastrointestinal symptoms in cystic fibrosis in the modulator era.NIHR Open Res. 2024 Feb 5;3:18. doi: 10.3310/nihropenres.13384.2. eCollection 2023. NIHR Open Res. 2024. PMID: 37881465 Free PMC article.
-
Antibiotic treatment for non-tuberculous mycobacteria lung infection in people with cystic fibrosis.Cochrane Database Syst Rev. 2025 Mar 27;3(3):CD016039. doi: 10.1002/14651858.CD016039. Cochrane Database Syst Rev. 2025. PMID: 40145528
-
Bronchoscopy-guided antimicrobial therapy for cystic fibrosis.Cochrane Database Syst Rev. 2024 May 3;5(5):CD009530. doi: 10.1002/14651858.CD009530.pub5. Cochrane Database Syst Rev. 2024. PMID: 38700027 Free PMC article.
-
Vanzacaftor-tezacaftor-deutivacaftor versus elexacaftor-tezacaftor-ivacaftor in individuals with cystic fibrosis aged 12 years and older (SKYLINE Trials VX20-121-102 and VX20-121-103): results from two randomised, active-controlled, phase 3 trials.Lancet Respir Med. 2025 Mar;13(3):256-271. doi: 10.1016/S2213-2600(24)00411-9. Epub 2025 Jan 2. Lancet Respir Med. 2025. PMID: 39756424 Free PMC article. Clinical Trial.
References
-
- World Health Organization . World Health Organization Bacterial Priority List. World Health Organization; Geneva, Switzerland: 2024.
Publication types
LinkOut - more resources
Full Text Sources
