

Effects of pulmonary rehabilitation combined with inspiratory muscle training on lung function and exercise capacity in older patients with COPD: a systematic review and meta-analysis
- PMID: 40703265
- PMCID: PMC12285735
- DOI: 10.3389/fmed.2025.1621375
Effects of pulmonary rehabilitation combined with inspiratory muscle training on lung function and exercise capacity in older patients with COPD: a systematic review and meta-analysis
Abstract
Background: Pulmonary rehabilitation is central to COPD management, with inspiratory muscle training (IMT) as a key component. However, evidence is inconsistent on whether combining PR with IMT offers added benefits for older COPD patients.
Objective: To evaluate the comparative effects of PR combined with IMT versus PR alone on key outcomes in older COPD patients, including quality of life [St. George's Respiratory Questionnaire (SGRQ)], exercise tolerance [6-min walk distance (6MWD)], respiratory muscle strength [maximal inspiratory pressure (PImax)], and pulmonary function metrics (FEV1, FEV1%).
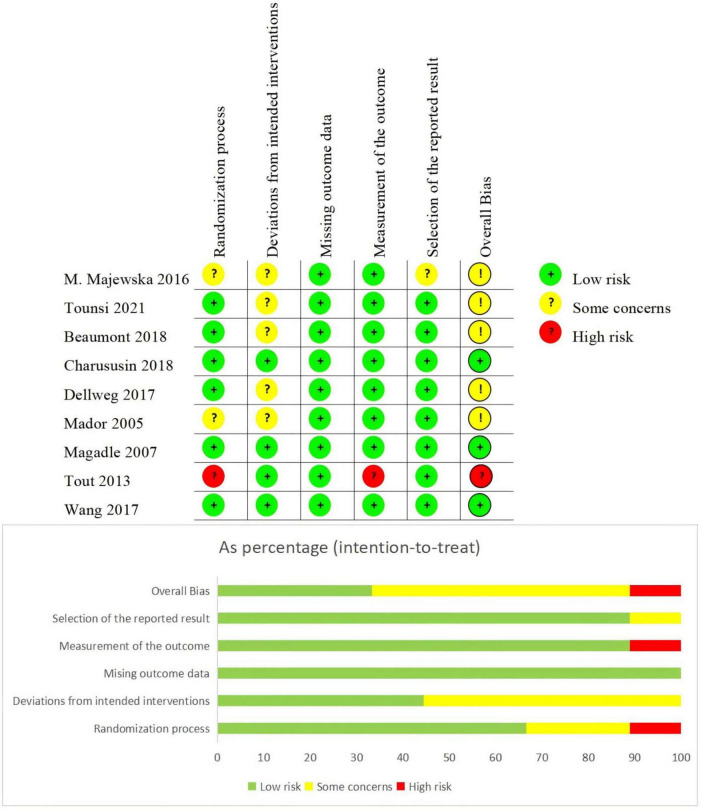
Methods: A systematic search of PubMed, EMBASE, Web of Science, and the Cochrane Library (January 2005-January 2025) identified randomized controlled trials (RCTs) meeting criteria: (1) participants were ≥ 55 years old with GOLD stage II-IV COPD; (2) interventions compared PR combined with IMT versus PR alone; (3) outcomes included PImax, FEV1, FEV1%, SGRQ, and 6MWD. Non-English and animal studies were excluded. Risk of bias was assessed using Cochrane RoB 2.0, and the certainty of evidence was evaluated via the GRADEpro 3.6.1.
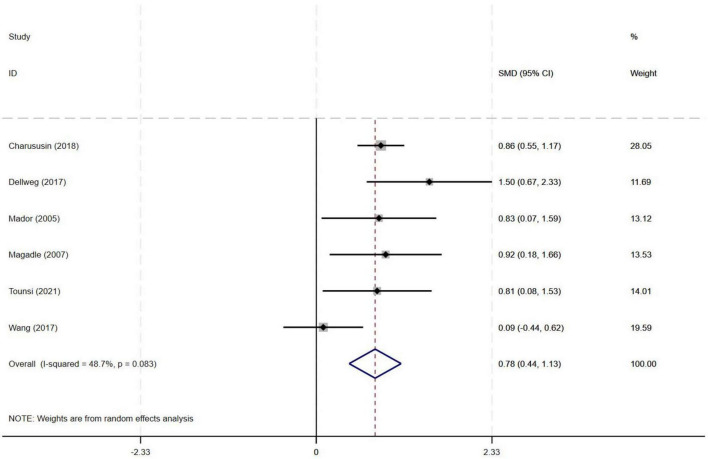
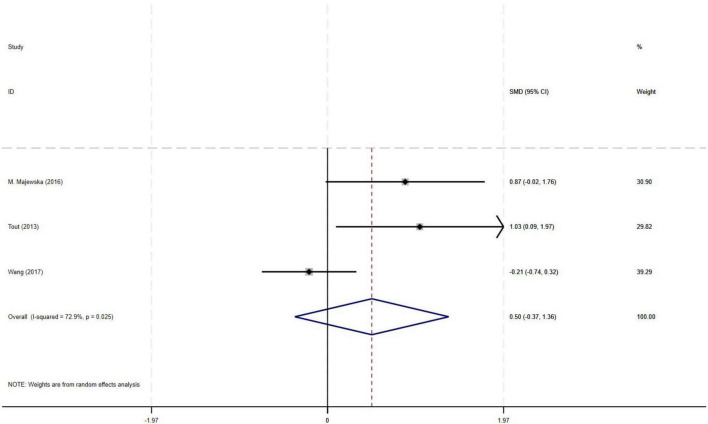
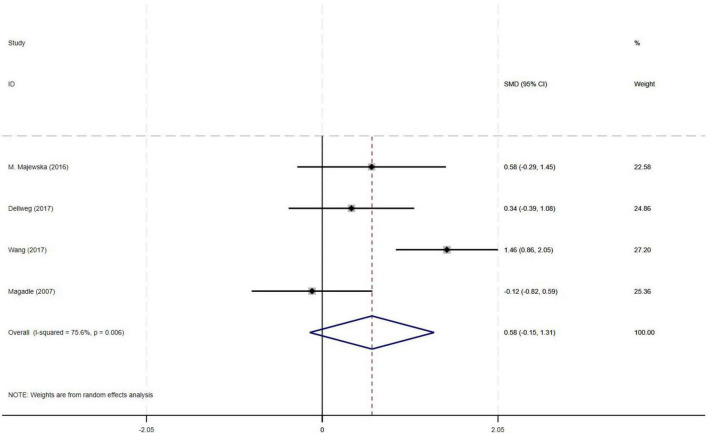
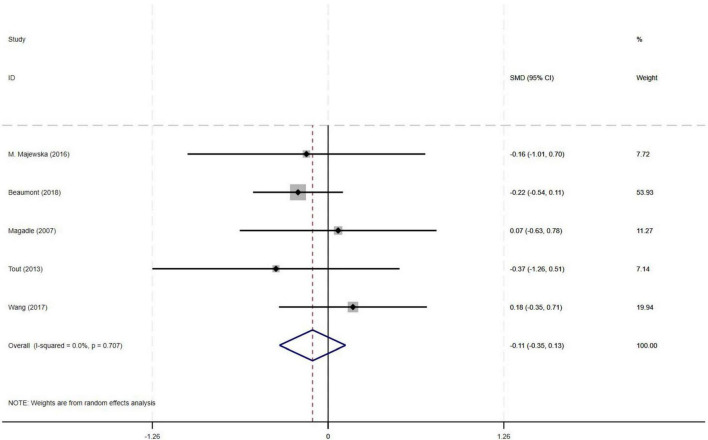
Results: Nine RCTs (582 patients) were included. Compared with PR alone, PR combined with IMT did not improve 6MWD (SMD = 0.15, 95% CI: -0.11-0.42; low-quality evidence) or SGRQ scores (SMD = -0.19, 95% CI: -0.38-0.01, low-quality evidence). PImax improved moderately (SMD = 0.78, 95% CI: 0.44-1.13, I2 = 48.7%, low-quality evidence). FEV1 and FEV1% trended upward (SMD = 0.50 and 0.58, respectively) but showed high heterogeneity (FEV1: I2 = 72.9%, p = 0.025, very low-quality evidence; FEV1%: I2 = 75.6%, p = 0.006, low-quality evidence), precluding significance. Subgroup analyses showed significant PImax improvements in interventions lasting ≥ 12 weeks (SMD = 0.866, 95% CI: 0.579-1.153; I2 = 0%) or with weekly cumulative durations ≥ 180 min (SMD = 0.922, 95% CI: 0.666-1.177; I2 = 0%), with no 6MWD benefits in any subgroup.
Conclusion: Low-quality evidence indicates that PR combined with IMT improves respiratory muscle strength (PImax) in older COPD patients versus PR alone, with no significant benefit for exercise capacity (6MWD) or lung function. For older COPD patients, ≥ 12-week PR combined with IMT interventions (sessions > 60 min; weekly duration ≥ 180 min) may enhance PImax.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD420251010168, CRD420251010168.
Keywords: COPD; exercise capacity; inspiratory muscle training; pulmonary function; pulmonary rehabilitation.
Copyright © 2025 Xie, Zhu, Wang, Mo, Shi, Liang, Ren, Bai and Nie.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
![Forest plot showing standardized mean differences with 95% confidence intervals for several studies: Tounsi (2021), Beaumont (2018), Tout (2013), Charususin (2018), Dellweg (2017), Mador (2005), Magadle (2007), and Wang (2017). Each study's weight is indicated, with a summary diamond representing overall effect at 0.15 [-0.11, 0.42]. Weights use random effects analysis.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/01ec/12285735/e588d27065fc/fmed-12-1621375-g003.jpg)
Similar articles
-
Inspiratory muscle training, with or without concomitant pulmonary rehabilitation, for chronic obstructive pulmonary disease (COPD).Cochrane Database Syst Rev. 2023 Jan 6;1(1):CD013778. doi: 10.1002/14651858.CD013778.pub2. Cochrane Database Syst Rev. 2023. PMID: 36606682 Free PMC article.
-
Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2016 Dec 8;12(12):CD005305. doi: 10.1002/14651858.CD005305.pub4. Cochrane Database Syst Rev. 2016. PMID: 27930803 Free PMC article.
-
Pulmonary rehabilitation versus usual care for adults with asthma.Cochrane Database Syst Rev. 2022 Aug 22;8(8):CD013485. doi: 10.1002/14651858.CD013485.pub2. Cochrane Database Syst Rev. 2022. PMID: 35993916 Free PMC article.
-
Pulmonary rehabilitation for chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2015 Feb 23;2015(2):CD003793. doi: 10.1002/14651858.CD003793.pub3. Cochrane Database Syst Rev. 2015. PMID: 25705944 Free PMC article.
-
Interventions to improve adherence to pharmacological therapy for chronic obstructive pulmonary disease (COPD).Cochrane Database Syst Rev. 2021 Sep 8;9(9):CD013381. doi: 10.1002/14651858.CD013381.pub2. Cochrane Database Syst Rev. 2021. PMID: 34496032 Free PMC article.
References
-
- Chen S, Kuhn M, Prettner K, Yu F, Yang T, Bärnighausen T, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: A health-augmented macroeconomic modelling study. Lancet Glob Health. (2023) 11:e1183–93. 10.1016/s2214-109x(23)00217-6 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials