

Three case reports of pulmonary mucormycosis with a review of the literature
- PMID: 40703293
- PMCID: PMC12283752
- DOI: 10.3389/fmed.2025.1580912
Three case reports of pulmonary mucormycosis with a review of the literature
Abstract
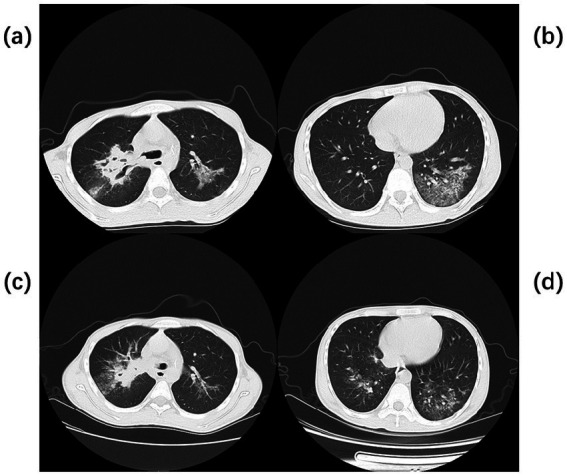
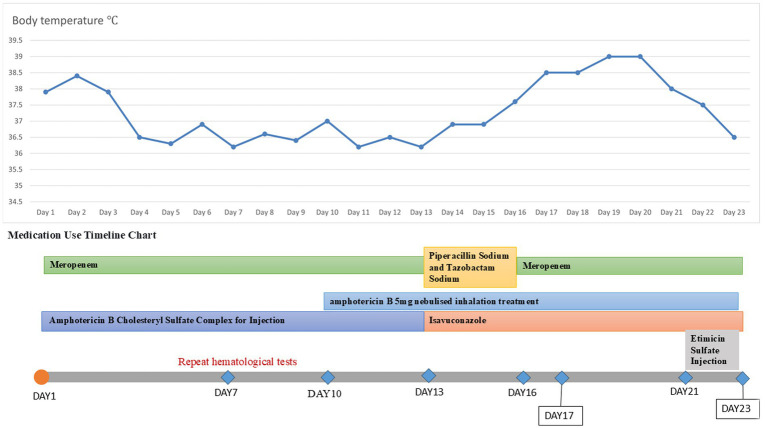
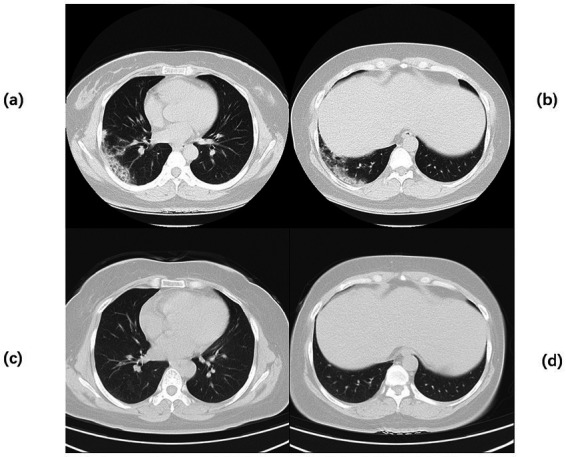
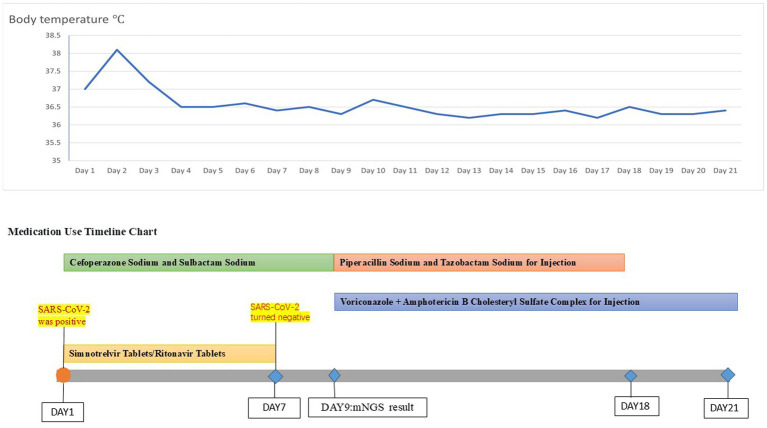
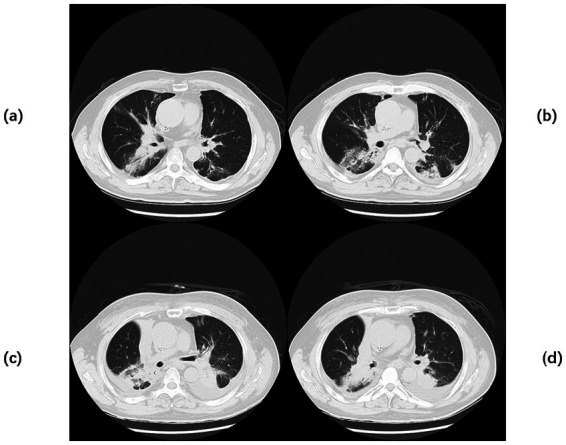
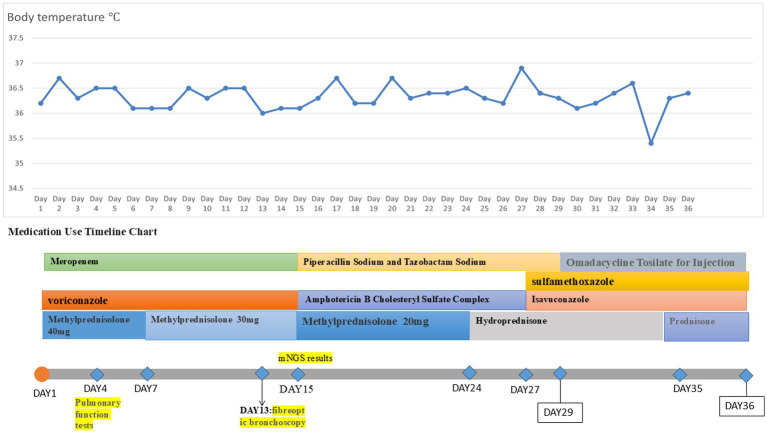
Pulmonary mucormycosis (PM) is an invasive and life-threatening fungal infection that predominantly affects immunocompromised individuals. This study thoroughly examined the disease through three case reports and a literature review. Case 1 involved a patient with type 1 diabetes mellitus diagnosed through bronchoscopic histopathology, who succumbed despite a combination of oral isavuconazole, nebulized amphotericin B, and intravenous amphotericin B cholesteryl sulfate complex. Case 2 involved a patient with follicular non-Hodgkin lymphoma who had a concurrent coronavirus disease 2019 (COVID-19) infection, which was confirmed through metagenomic next-generation sequencing (mNGS) of bronchoalveolar lavage fluid (BALF). The patient experienced clinical improvement following sequential intravenous voriconazole, amphotericin B cholesteryl sulfate complex, and oral isavuconazole. Case 3 involved a patient diagnosed with mNGS in a lung cancer patient with chronic obstructive pulmonary disease, who showed poor therapeutic response to combined intravenous voriconazole, amphotericin B cholesteryl sulfate complex, and oral isavuconazole, resulting in fatal outcomes. Literature synthesis revealed mortality rates of 28.3% with antifungal monotherapy compared to 23.7% when antifungal monotherapy was combined with bronchoscopic intervention; the mortality rate for antifungal-surgical combination therapy was 9%. Notably, all 13 patients receiving multimodal treatment (antifungals, bronchoscopy, and surgery) survived. These findings underscore that combination therapy integrating pharmacotherapy, bronchoscopic intervention, and surgical resection demonstrated significantly superior survival outcomes compared to monotherapy.
Keywords: amphotericin B; bronchoalveolar lavage; case report; literature review; pulmonary mucormycosis.
Copyright © 2025 Zhang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Alexander BD, Lamoth F, Heussel CP, Prokop CS, Desai SR, Morrissey CO, et al. Guidance on imaging for invasive pulmonary aspergillosis and mucormycosis: from the imaging working Group for the Revision and Update of the consensus definitions of fungal disease from the EORTC/MSGERC. Clin Infect Dis. (2021) 72:S79–88. doi: 10.1093/cid/ciaa1855, PMID: - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources