

Palliative Care Specialist Use Among Medicare Decedents Who Had Poor-Prognosis Cancers
- PMID: 40705332
- PMCID: PMC12290731
- DOI: 10.1001/jamanetworkopen.2025.22886
Palliative Care Specialist Use Among Medicare Decedents Who Had Poor-Prognosis Cancers
Abstract
Importance: Palliative care (PC) use patterns may have changed in recent years due to increased adoption of telehealth and the availability of more advanced practice clinicians who specialize in PC delivery.
Objective: To describe changes in the use of specialty PC during the last year of life among Medicare beneficiaries who had cancers with poor prognoses (cancers that commonly caused death, rare cancers with high mortality rates, or solid tumors with concurrent nonlymphatic metastases; hereinafter termed poor-prognosis cancers).
Design, setting, and participants: This retrospective cohort study includes all US Medicare fee-for-service beneficiaries who died from poor-prognosis cancers between January 1, 2018, and December 31, 2023, and received care in hospital and outpatient settings.
Exposures: Encounters with a PC specialist.
Main outcomes and measures: The primary outcome was the proportion of decedents with any specialty PC encounter in their last year of life. Secondary outcomes included mean number of PC encounters among decedents with at least 1 encounter with a PC specialist and telehealth use. PC specialists were clinicians who self-identified as a PC specialist or were clinicians with 80% or more of their Medicare encounters focused on PC.
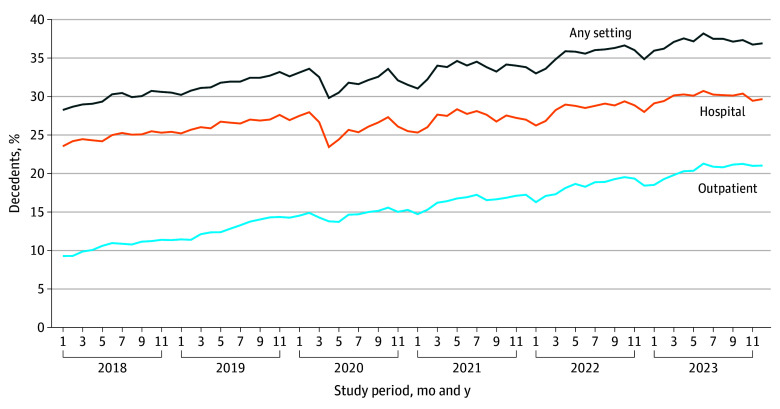
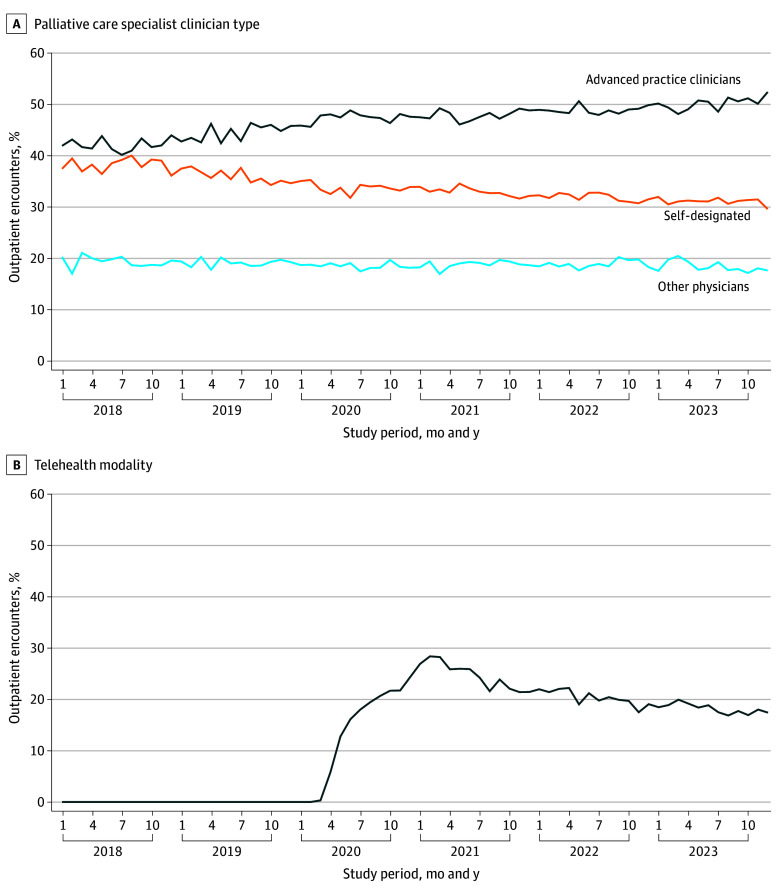
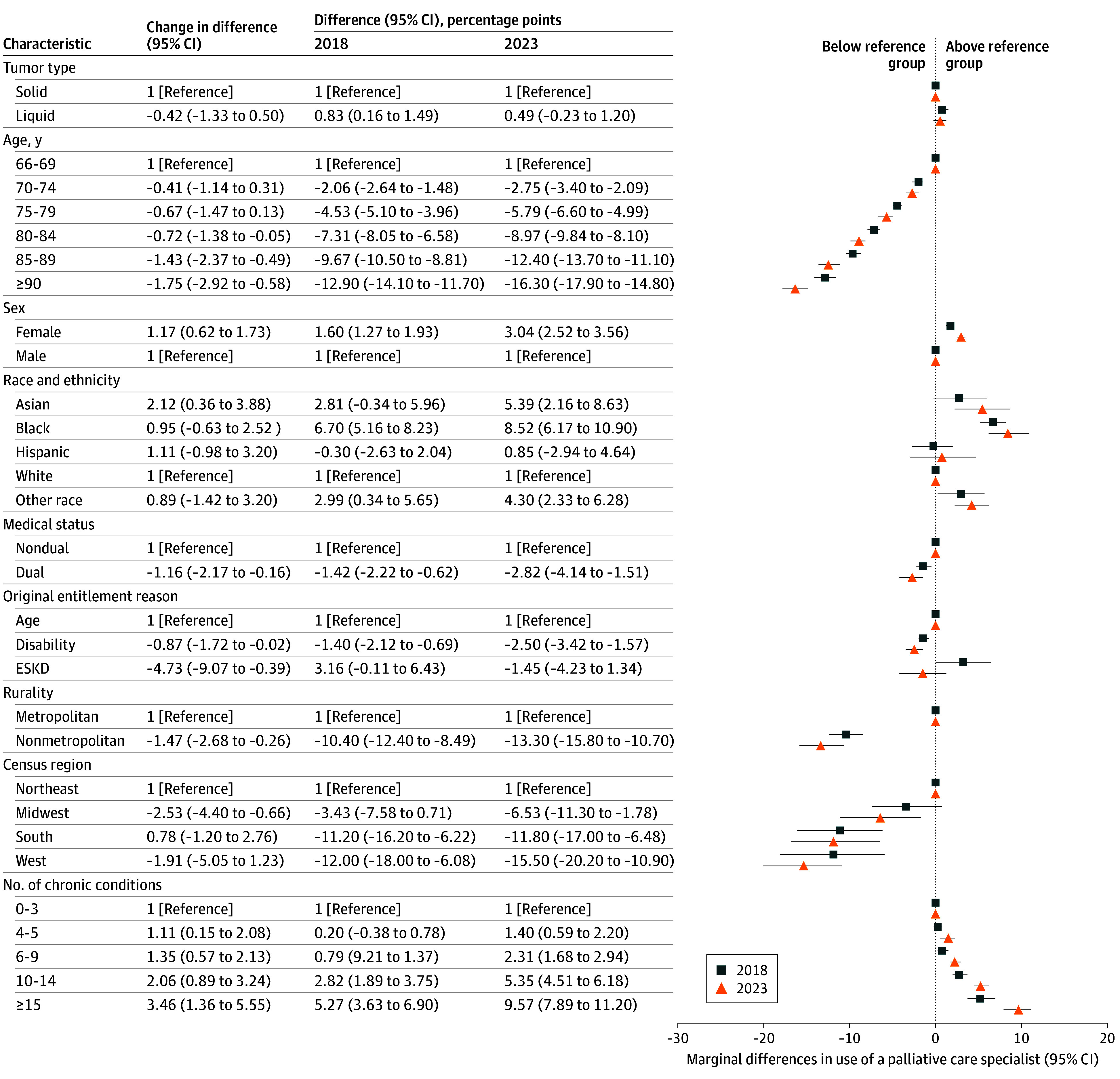
Results: The cohort included 1 508 103 decedents (mean [SD] age, 79.6 [8.0] years; 54.6% male) with poor-prognosis cancers. Between 2018 and 2023, the proportion of decedents with at least 1 PC encounter increased from 29.84% to 37.21% (adjusted change, 7.21 [95% CI, 6.30-8.12] percentage points; relative change, 24.2%). The proportion who received outpatient PC increased from 10.66% to 20.56% (adjusted change, 9.41 [95% CI, 8.33-10.48] percentage points; relative change, 88.2%). In 2023, 22.84% of all decedents received PC from advanced practice clinicians vs 15.60% by self-designated PC physicians and 9.92% by other physicians. Telehealth was used for 18.2% of all outpatient palliative care encounters in 2023. Decedent characteristics associated with not receiving specialty PC included older age, lower income, and living in nonmetropolitan areas.
Conclusions and relevance: In this cohort study of decedents who had poor-prognosis cancers, an increasing proportion received any specialty PC. Advanced practice specialists were the most common clinician type who delivered specialty PC, and telehealth was used for a substantial proportion of outpatient visits. Despite these changes, only a minority of patients received specialty PC, and low use of specialty PC among certain subpopulations persisted, suggesting that different strategies are needed to overcome these barriers.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
