

Digital Interventions for Cognitive Dysfunction in Patients With Stroke: Systematic Review and Meta-Analysis
- PMID: 40705404
- PMCID: PMC12288705
- DOI: 10.2196/73687
Digital Interventions for Cognitive Dysfunction in Patients With Stroke: Systematic Review and Meta-Analysis
Abstract
Background: In recent years, digital technologies have shown possibilities for improving cognitive function after stroke, but their effectiveness and treatment options vary, the optimal treatment remains unclear, and the current evidence is somewhat contradictory.
Objective: This study aimed to evaluate the efficacy of various digital interventions in improving poststroke cognitive function and provide evidence-based support for clinical decision-making.
Methods: A systematic search was conducted across PubMed, Web of Science, Cochrane Library, Scopus, Embase, and CNKI databases from their inception to January 2025, with no restrictions on language or publication year. Randomized controlled trials evaluating digital interventions (eg, virtual reality [VR], computer-assisted cognitive therapy [CACT], and robot-assisted therapy [RAT]) for poststroke cognitive impairment in adults (aged≥18 y) were included. Eligible studies reported outcomes measured by the Montreal Cognitive Assessment (MoCA) or the Mini-Mental State Examination (MMSE), with cognitive improvement quantified through pre- to postintervention scores. Multiple researchers independently extracted data. Network meta-analysis was performed using R software, incorporating consistency or inconsistency models (based on Deviance Information Criterion differences), random-effects models, and I² statistics to assess heterogeneity. Sources of heterogeneity were analyzed through sensitivity analyses, subgroup analyses, and meta-regression. Intervention efficacy was ranked using Surface Under the Cumulative Ranking Curve (SUCRA) values. Robustness and consistency were validated via Egger test, sensitivity analyses, and node-splitting methods. Evidence quality was assessed using the Grading of Recommendations Assessment, Development, and Evaluation framework.
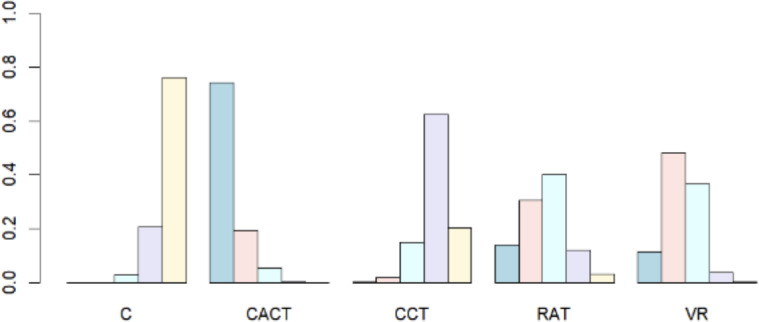
Results: A total of 2128 articles were retrieved, with 27 meeting the inclusion criteria. Compared to conventional rehabilitation or care (C), CACT demonstrated significant superiority in MoCA scores (mean difference [MD]=3.03, 95% CI 1.69 to 4.38; SUCRA=91.53%); while cognitive training (CCT) demonstrated no statistical difference (MD=0.70, 95% CI -0.88 to 2.28). The ordering is CACT>VR>RAT>CCT. For MMSE scores, RAT ranked highest in efficacy (MD=5.99, 95% CI 3.20 to 8.79; SUCRA=99.44%); whereas both VR (MD=1.34, 95% CI -0.94 to 3.62) and CCT (MD=1.12, 95% CI -1.46 to 3.69) showed no significant improvement. The ordering is RAT>CACT>CCT>VR.
Conclusions: Digital therapies are effective in improving cognitive functioning in patients post stroke. CACT showed superior efficacy on the MoCA (emphasizing executive functioning), while RAT had the highest efficacy in the MMSE (focusing on basic cognition), suggesting different domain-specific effects. However, caution is warranted due to the heterogeneity of the included studies, risk of bias, and limited sample sizes in some studies. Future research should focus on optimizing intervention protocols, integrating neuromodulation or traditional rehabilitation techniques, and exploring cost-effective clinical implementation strategies.
Keywords: cognitive impairment; cognitive training; computer-assisted therapy; robotics; stroke; virtual reality.
©Chen Wang, Min Liu. Originally published in the Journal of Medical Internet Research (https://www.jmir.org).
Conflict of interest statement
Figures








References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
