

Emergency department visits among rural and urban older adults: disparities in ambulatory and emergency care sensitive conditions
- PMID: 40707938
- PMCID: PMC12291402
- DOI: 10.1186/s12913-025-13161-2
Emergency department visits among rural and urban older adults: disparities in ambulatory and emergency care sensitive conditions
Abstract
Background: Older adults in rural geographies may be uniquely vulnerable to difficulty accessing outpatient care, and therefore more reliant on emergency department (ED) care. We compared ED utilization for ambulatory care sensitive conditions (ACSCs) and emergency care sensitive conditions (ECSCs) among rural and urban Medicare beneficiaries.
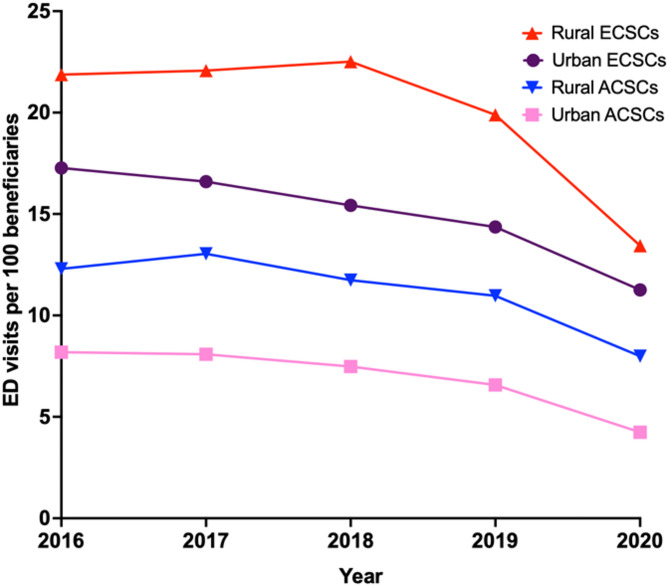
Methods: We conducted a pooled cross-sectional analysis of 2016-2020 Medicare Current Beneficiary Survey data, assessing ED visitation rates for ACSCs and ECSCs. We present ED visit rates per 100 beneficiary-years and estimated logistic regression models to quantify the odds of having any ED visit, any ACSC-related ED visit, or any ECSC-related ED visit in a given year among older adults in rural and urban areas, adjusting for sociodemographic and health characteristics.
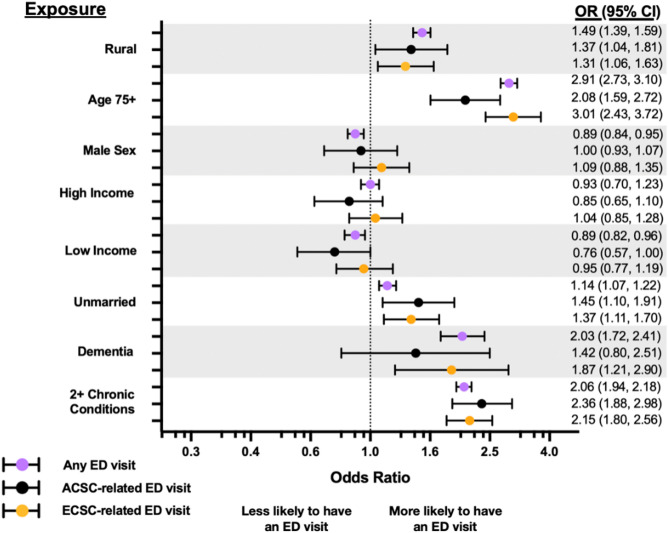
Results: Our sample included 70,830 beneficiary-years, with 17,052 (24.1%) being from beneficiaries residing in rural areas. Rural beneficiaries had higher ED visit rates, with a weighted mean (SD) of 59.2 ED visits (14.1) per 100 beneficiary-years across study years, 11.5 (1.3) for ACSC-related, and 20.6 (3.5) for ECSC-related visits, compared to 43.2 (9.2), 7.2 (0.9), and 15.2 (1.9) ED visits, respectively, for urban beneficiary-years. In adjusted models, rural beneficiaries had a 49% higher odds of having an ED visit (OR: 1.49, 95% CI: 1.40-1.59), a 30% higher odds of an ACSC-related ED visit (OR: 1.30, 95% CI: 1.04-1.64), and a 26% higher odds of an ECSC-related ED visit (OR: 1.26, 95% CI: 1.05-1.50) within a given year when compared to urban counterparts.
Conclusions: Rural Medicare beneficiaries consistently showed higher ED utilization for ACSCs and ECSCs compared to urban beneficiaries, highlighting potential disparities in healthcare access and a need for targeted or policy-based interventions.
Keywords: Ambulatory care sensitive conditions; Emergency care sensitive conditions; Emergency department; Older adults; Rural.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The primary author’s Institutional Review Board determined that this study was exempt secondary research for which patient informed consent was not required. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Gruneir A, Silver MJ, Rochon PA. Emergency department use by older adults: a literature review on trends, appropriateness, and consequences of unmet health care needs. Med Care Res Rev. 2011;68(2):131–55. - PubMed
-
- Pines JM, Mullins PM, Cooper JK, Feng LB, Roth KE. National trends in emergency department use, care patterns, and quality of care of older adults in the united States. J Am Geriatr Soc. 2013;61(1):12–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
