

Effects and neural mechanisms of a brain-computer interface-controlled soft robotic glove on upper limb function in patients with subacute stroke: a randomized controlled fNIRS study
- PMID: 40707971
- PMCID: PMC12288246
- DOI: 10.1186/s12984-025-01704-x
Effects and neural mechanisms of a brain-computer interface-controlled soft robotic glove on upper limb function in patients with subacute stroke: a randomized controlled fNIRS study
Abstract
Background and purpose: The brain-computer interface-based soft robotic glove (BCI-SRG) holds promise for upper limb rehabilitation in subacute stroke patients, yet its efficacy and neural mechanisms are unclear. This study aimed to investigate the therapeutic effects and neural mechanisms of BCI-SRGs by functional near-infrared spectroscopy (fNIRS).
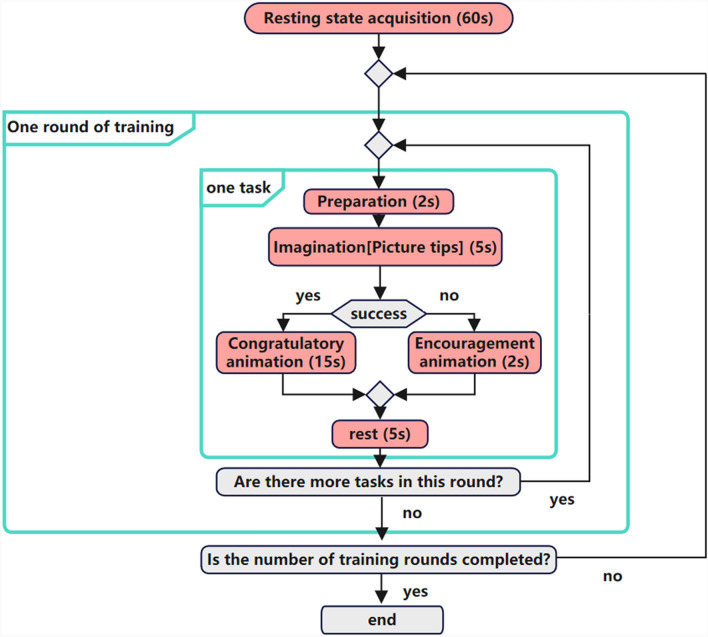
Methods: Forty subacute stroke patients with left-sided hemiparesis were randomized into the BCI-SRG (n = 20) and soft robotic glove (SRG) (n = 20) groups. Both groups received 20 sessions of intervention over 4 weeks in addition to conventional rehabilitation. The BCI-SRG group was trained using a soft robotic glove controlled by a brain‒computer interface (BCI), whereas the SRG group used the same soft robotic glove without BCI control. The clinical outcomes included the Action Research Arm Test (ARAT), the Fugl-Meyer Assessment Upper Limb (FMA-UL), and Modified Barthel Index (MBI) scores. In addition, fNIRS was used to explore potential clinical brain mechanisms. All assessments were performed before treatment and after 4 weeks of treatment.
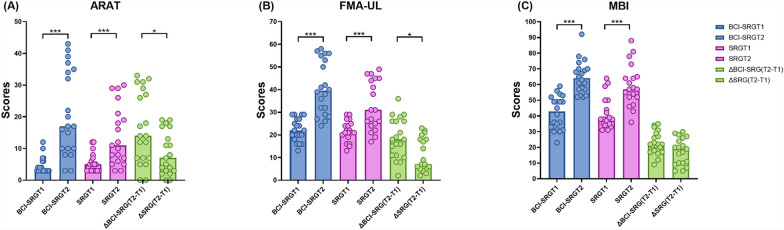
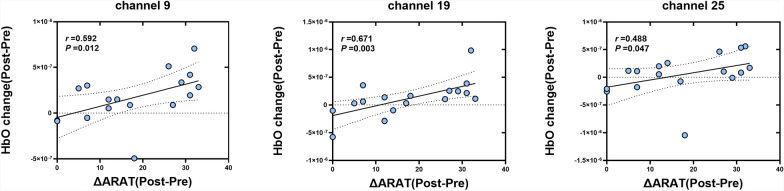
Results: A total of 39 participants completed the intervention and clinical assessments (BCI-SRG: n = 20; SRG: n = 19). Compared with the SRG group, the BCI-SRG group showed greater improvements in the ARAT (Z = - 2.139, P = 0.032) and FMA-UL (Z = - 2.588, P = 0.010), with no notable difference in the MBI (Z = - 1.843, P = 0.065). fNIRS data were available for 35 participants (BCI-SRG: n = 17; SRG: n = 18). Within-group comparisons revealed significant postintervention increases in cortical activation in the bilateral sensorimotor cortex (SMC) and medial prefrontal cortex (MPFC) in the BCI-SRG group, whereas no significant changes were observed in the SRG group. Between-group comparisons further revealed significantly greater changes in HbO concentrations in the BCI-SRG group than in the SRG group across the same cortical regions. Moreover, changes in prefrontal activation (post-pre) were positively correlated with improvements in ARAT scores, with significant correlations observed in the left dorsal lateral prefrontal cortex (LDLPFC) (Ch9, r = 0.592, P = 0.012; Ch25, r = 0.488, P = 0.047) and right dorsal lateral prefrontal cortex (RDLPFC) (Ch19, r = 0.671, P = 0.003).
Conclusions: BCI-SRG training significantly enhances upper limb function and facilitates bilateral motor and sensory cortical reorganization. PFC activation is correlated with functional improvements, suggesting a potential mechanism underlying the benefits of rehabilitation in stroke patients.
Trial registration: This trial was registered under the Chinese Clinical Trial Registry (ChiCTR2400082786) and was retrospectively registered on April 8, 2024.
Keywords: Brain‒computer interface; Functional near-infrared spectroscopy; Soft robotic glove; Stroke; Upper limb.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Ethics Committee of Wuxi Central Rehabilitation Hospital (WXMHCIRB2024LLky018). All procedures followed were in accordance with the ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Competing interests: The authors declare no competing interests.
Figures



References
-
- Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet (London, England). 2011;377:1693–702. 10.1016/s0140-6736(11)60325-5. - PubMed
-
- Lieshout E, van de Port IG, Dijkhuizen RM, Visser-Meily JMA. Does upper limb strength play a prominent role in health-related quality of life in stroke patients discharged from inpatient rehabilitation? Top Stroke Rehabil. 2020;27:525–33. 10.1080/10749357.2020.1738662. - PubMed
-
- Teasell R. et al. Canadian Stroke Best Practice Recommendations: rehabilitation, Recovery, and Community Participation following Stroke. Part One: rehabilitation and Recovery Following Stroke; 6th Edition Update 2019. Int J Stroke Off J Int Stroke Soc. 2020;15:763–788. 10.1177/1747493019897843 - PubMed
Publication types
MeSH terms
Grants and funding
- No.Q202414/Youth Project of the Wuxi Municipal Health Commission
- No.2022YFC2009700/National Key Research & Development Program of China
- No.BE2023023-2/the Key Project of Jiangsu Province's Key Research and Development Program
- No.BE2023034/the Competitive Project of Jiangsu Province's Key Research and Development Program
- No.JBGS202414/Jiangsu Province Hospital clinical diagnosis and treatment of technological innovation "Open bidding for selecting the best candidates" project
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
