

CPAP improves regional lung strain rate and diaphragm velocity of relaxation in experimental self-inflicted lung injury
- PMID: 40707978
- PMCID: PMC12291241
- DOI: 10.1186/s13054-025-05536-y
CPAP improves regional lung strain rate and diaphragm velocity of relaxation in experimental self-inflicted lung injury
Abstract
Background: Strenuous respiratory effort has been proposed as a second hit in severe acute lung injury (ALI), introducing the concept of "patient self-inflicted lung injury" (P-SILI). In an experimental setting, noninvasive continuous positive airway pressure (CPAP) attenuates lung and diaphragmatic injury, but the underlying mechanisms remains elusive. Here we investigate the effects of noninvasive CPAP on global and regional lung strain and diaphragm velocity of contraction and relaxation in an experimental P-SILI model.
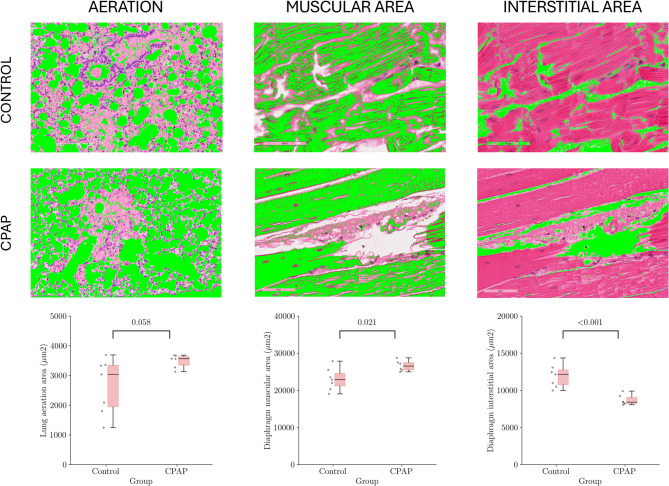
Methods: Lung injury was induced in Sprague Dawley rats through surfactant depletion followed by either three hours of standard oxygen therapy (Control group) or CPAP support (CPAP group). Subjects were assessed through inspiratory and expiratory muscle activation. Regional lung and diaphragmatic deformation amplitude (strain) and the rate of change (strain rate) maps were developed using a micro-computed tomography (µCT) scan. Morphometric tissue assessment was carried out to study biological damage.
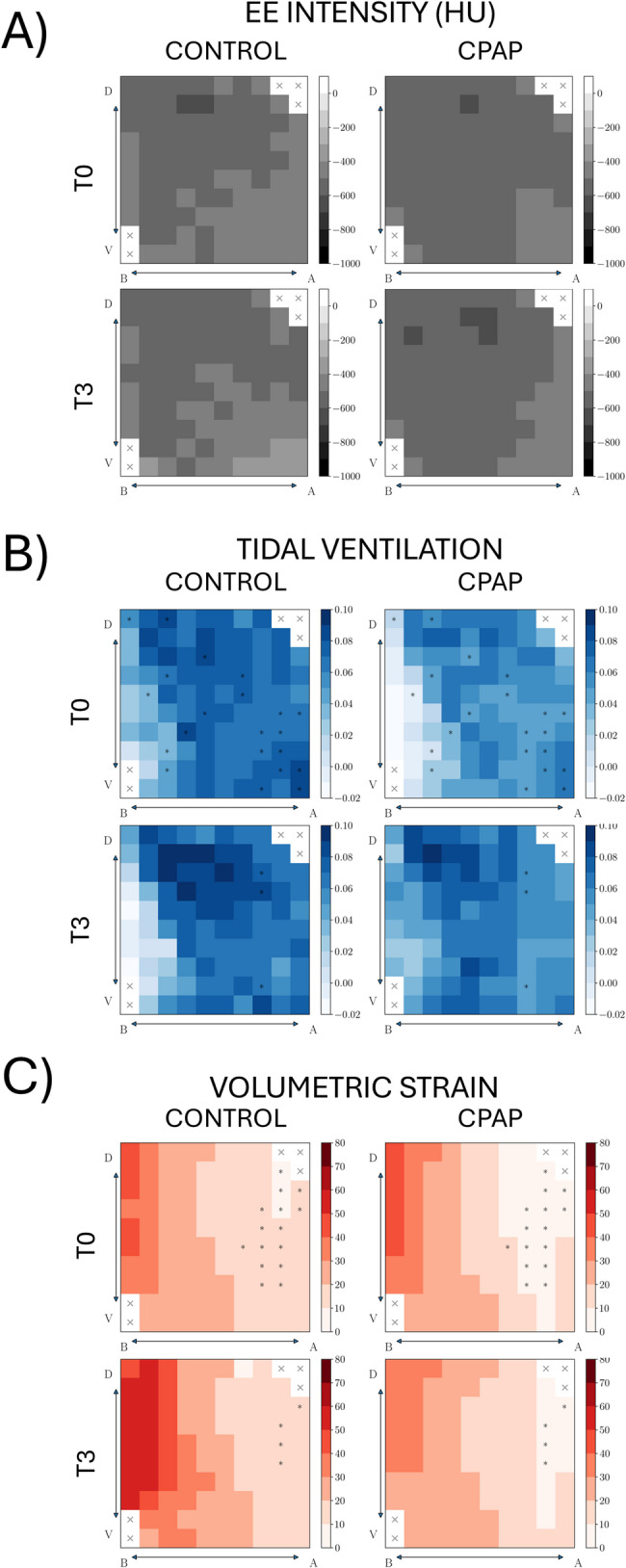
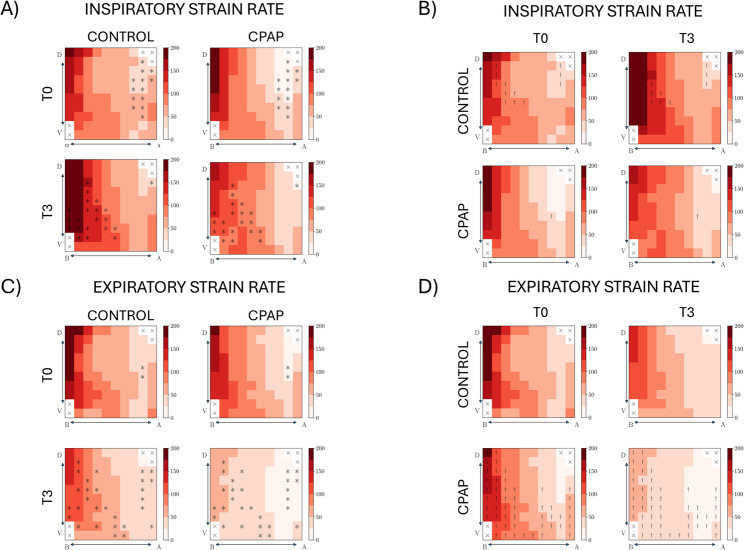
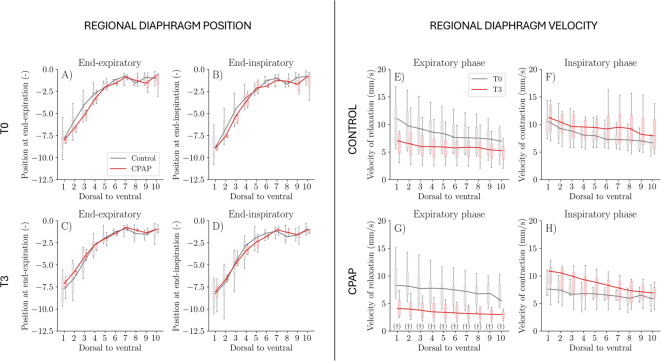
Results: Compared with the Control group, the CPAP group resulted in: (1) higher SpO2 and lower respiratory rate, nasal flaring, inspiratory and expiratory muscle activation, and minute ventilation at the end of the study; (2) lower global and regional tidal ventilation at the beginning of the study; (3) lower regional inspiratory and expiratory lung strain rate over time; and (4) higher muscle area in the diaphragm morphometric analysis. Furthermore, intragroup analysis showed that only the CPAP group reduced the inspiratory and expiratory muscle activation, the global and regional expiratory lung strain rate and the regional velocity of relaxation of the diaphragm over time.
Conclusions: Standard oxygen therapy resulted in worse patterns of lung strain rate and diaphragm velocity of relaxation, consistent with P-SILI and load-induced diaphragm injury. CPAP resulted in improved lung function, decreased lung strain rate, and diaphragmatic relaxation velocity throughout the respiratory cycle. We conclude that CPAP promotes biomechanical protection in injured lungs and diaphragm, more noticeably during the expiratory phase.
Keywords: Acute lung injury; Continuous positive airway pressure; Patient self-inflicted lung injury; Respiratory effort; Spontaneous breathing; Strain; Strain rate.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol was approved by the Universidad Andrés Bello Bioethics Committee, approval ID #05/2016 and #020/2017. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Ventilator Management(Archived).2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28846232 Free Books & Documents.
-
Effects of Noninvasive Respiratory Support on Ventilation Distribution During Spontaneous Breathing Sedation in Preschool/School-Aged Children: An Electrical Impedance Tomography Study.Paediatr Anaesth. 2025 Jul;35(7):562-572. doi: 10.1111/pan.15098. Epub 2025 Mar 22. Paediatr Anaesth. 2025. PMID: 40119601 Free PMC article. Clinical Trial.
-
Non-invasive ventilation for cystic fibrosis.Cochrane Database Syst Rev. 2017 Feb 20;2(2):CD002769. doi: 10.1002/14651858.CD002769.pub5. Cochrane Database Syst Rev. 2017. PMID: 28218802 Free PMC article.
-
Continuous positive airway pressure (CPAP) for acute bronchiolitis in children.Cochrane Database Syst Rev. 2022 Apr 4;4(4):CD010473. doi: 10.1002/14651858.CD010473.pub4. Cochrane Database Syst Rev. 2022. PMID: 35377462 Free PMC article.
-
Noninvasive positive pressure ventilation for acute respiratory failure following upper abdominal surgery.Cochrane Database Syst Rev. 2015 Oct 5;2015(10):CD009134. doi: 10.1002/14651858.CD009134.pub2. Cochrane Database Syst Rev. 2015. PMID: 26436599 Free PMC article.
References
-
- Yoshida T, Uchiyama A, Matsuura N, Mashimo T, Fujino Y. The comparison of spontaneous breathing and muscle paralysis in two different severities of experimental lung injury. Crit Care Med. 2013;41:536–45. - PubMed
-
- Yoshida T, Uchiyama A, Matsuura N, Mashimo T, Fujino Y. Spontaneous breathing during lung-protective ventilation in an experimental acute lung injury model: high transpulmonary pressure associated with strong spontaneous breathing effort May worsen lung injury. Crit Care Med. 2012;40:1578–85. - PubMed
-
- Brochard L, Slutsky A, Pesenti A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am J Respir Crit Care Med. 2017;195:438–42. - PubMed
MeSH terms
Grants and funding
- Fondecyt Regular 1220322/Agencia Nacional de Investigación y Desarrollo, ANID Chile
- Fondecyt Regular 1220322/Agencia Nacional de Investigación y Desarrollo, ANID Chile
- Fondecyt Regular 1220322/Agencia Nacional de Investigación y Desarrollo, ANID Chile
- Fondecyt Regular 1220465/Agencia Nacional de Investigación y Desarrollo
LinkOut - more resources
Full Text Sources
