

Vaccination as a strategy for Chlamydia trachomatis control: a global mathematical modeling analysis
- PMID: 40708051
- PMCID: PMC12291290
- DOI: 10.1186/s44263-025-00181-7
Vaccination as a strategy for Chlamydia trachomatis control: a global mathematical modeling analysis
Abstract
Background: Chlamydia trachomatis (CT) is among the most common sexually transmitted infections and is associated with substantial health and economic burdens. Vaccination may offer a promising strategy for its global control.
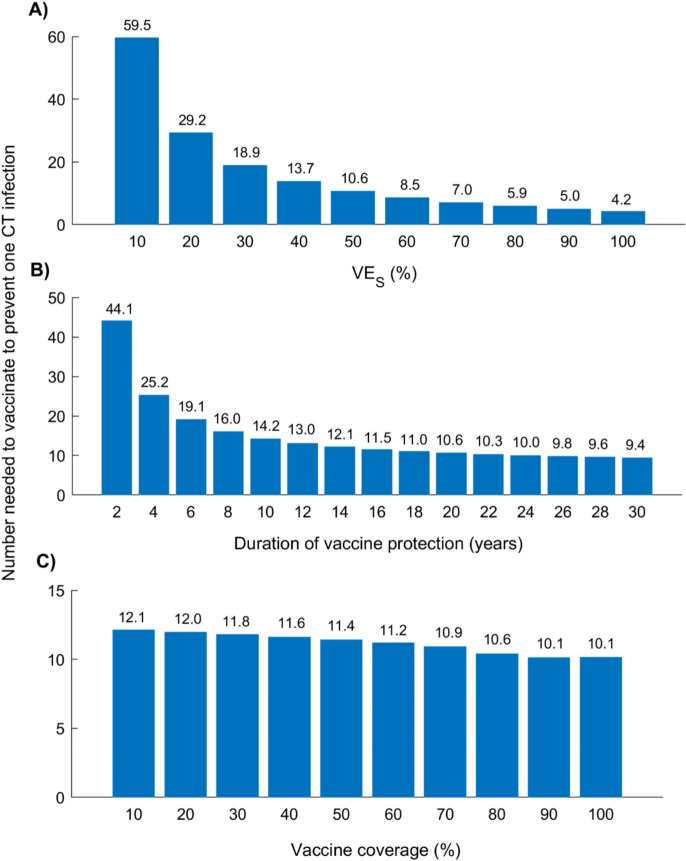
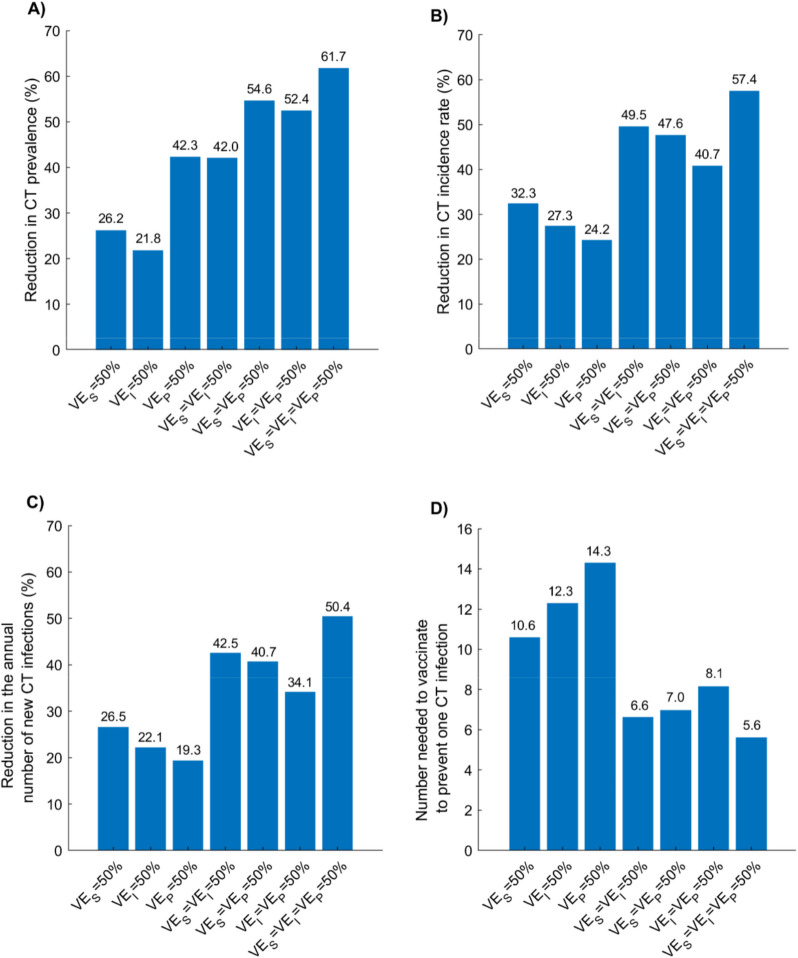
Methods: A deterministic, age-structured mathematical model was applied to assess the global impact of a hypothetical CT vaccine. The analysis explored a range of assumptions for vaccine efficacy against infection acquisition ( ), duration of protection, and coverage, across both adult catch-up and adolescent-targeted vaccination strategies.
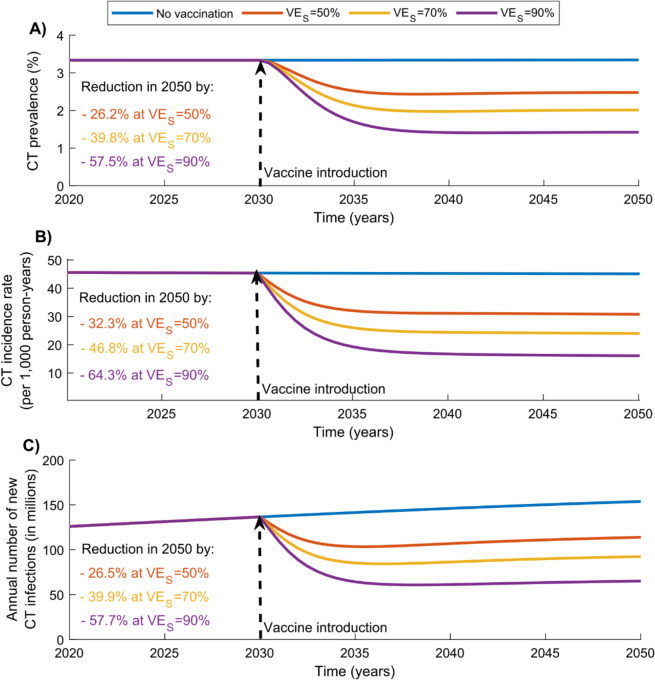
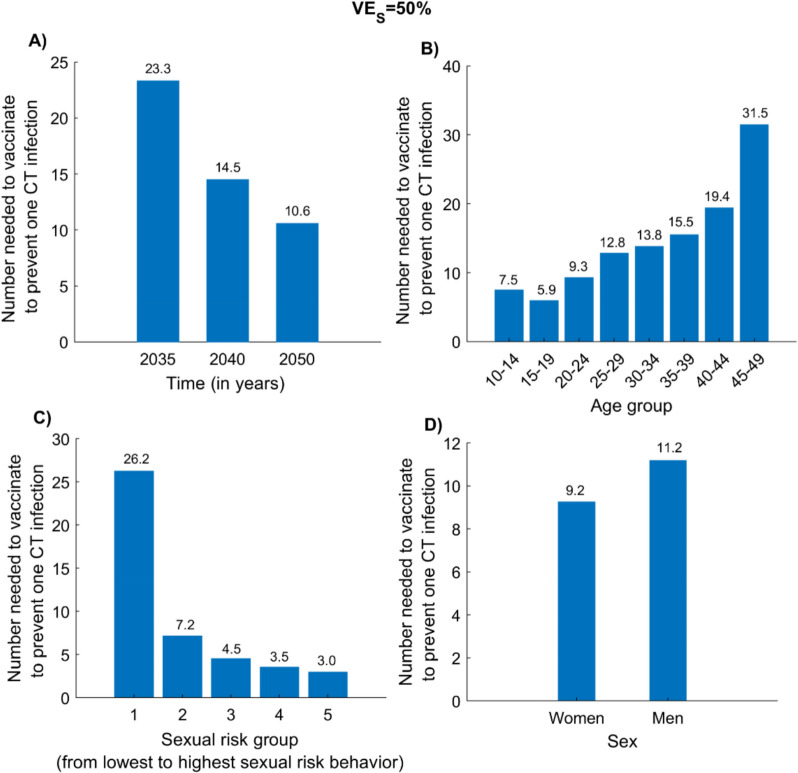
Results: Vaccinating individuals aged 15-49 years beginning in 2030 with a vaccine of and 20-year protection, scaled to 80% coverage by 2040, reduced global CT prevalence, incidence rate, and annual new infections in 2050 by 26.2%, 32.3%, and 26.5%, respectively. Cumulatively, 717 million infections were averted by 2050. The number needed to vaccinate (NNV) to prevent one infection declined from 23.3 in 2035 to 10.6 in 2050, with variation across population groups: 5.9 for those aged 15-19 years, 7.5 for those aged 10-14 years, and 3.0 for high-risk groups. Vaccine impact increased with higher , longer protection duration, and inclusion of breakthrough effects on infectiousness and infection duration. While adolescent vaccination achieved substantial impact, its benefits accrued more slowly than those of adult-targeted strategies.
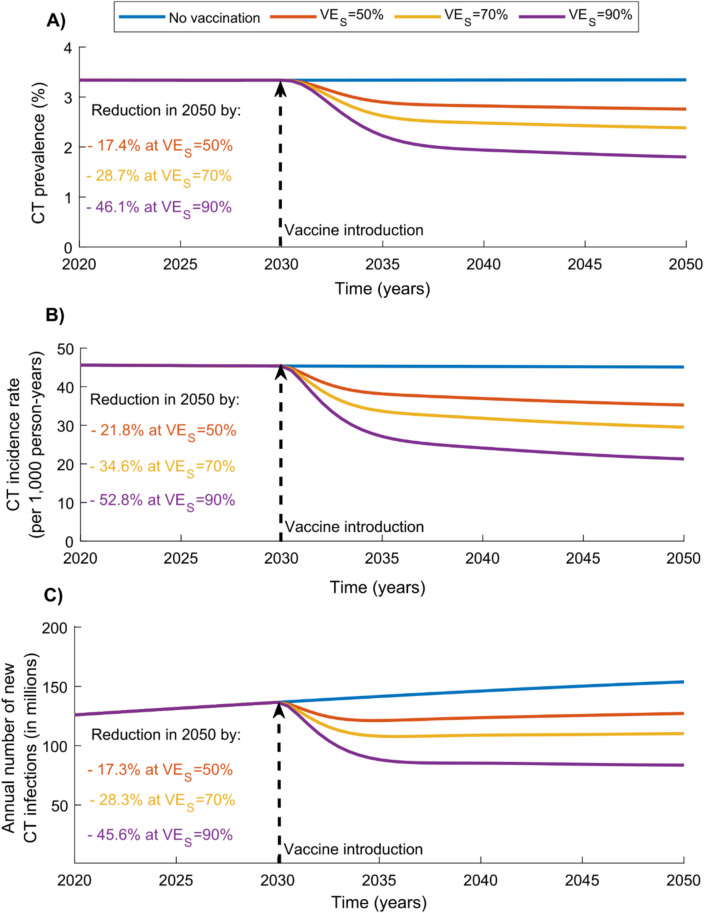
Conclusions: Vaccination against CT can substantially reduce global infection burden, even with moderate efficacy. Impact is enhanced by targeted strategies, with adolescent vaccination aiding long-term control and catch-up programs ensuring immediate benefit. These findings highlight the urgency of vaccine development and integration into public health efforts.
Keywords: Cost-effectiveness; Global health; Number needed to vaccinate; Sexually transmitted infection; Transmission dynamics; Vaccine impact.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Immunogenicity and seroefficacy of pneumococcal conjugate vaccines: a systematic review and network meta-analysis.Health Technol Assess. 2024 Jul;28(34):1-109. doi: 10.3310/YWHA3079. Health Technol Assess. 2024. PMID: 39046101 Free PMC article.
-
Population-based interventions for reducing sexually transmitted infections, including HIV infection.Cochrane Database Syst Rev. 2004;(2):CD001220. doi: 10.1002/14651858.CD001220.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2011 Mar 16;(3):CD001220. doi: 10.1002/14651858.CD001220.pub3. PMID: 15106156 Updated.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors.Cochrane Database Syst Rev. 2018 May 9;5(5):CD009069. doi: 10.1002/14651858.CD009069.pub3. Cochrane Database Syst Rev. 2018. PMID: 29740819 Free PMC article.
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
References
-
- Rekart ML, Gilbert M, Meza R, Kim PH, Chang M, Money DM, Brunham RC. Chlamydia public health programs and the epidemiology of pelvic inflammatory disease and ectopic pregnancy. J Infect Dis. 2013;207(1):30–8. - PubMed
-
- Mishori R, McClaskey EL, WinklerPrins VJ. Chlamydia trachomatis infections: screening, diagnosis, and management. Am Fam Physician. 2012;86(12):1127–32. - PubMed
-
- McConaghy JR, Panchal B. Epididymitis: an overview. Am Fam Physician. 2016;94(9):723–6. - PubMed
Grants and funding
- ARG01-0522-230273/Qatar Research Development and Innovation Council
- ARG01-0522-230273/Qatar Research Development and Innovation Council
- Biostatistics, Epidemiology, and Biomathematics Research Core/Weill Cornell Medicine - Qatar
- Biostatistics, Epidemiology, and Biomathematics Research Core/Weill Cornell Medicine - Qatar
LinkOut - more resources
Full Text Sources