

Shield ulcer in keratoconus in the absence of atopic or vernal kerato-conjunctivitis
- PMID: 40708598
- PMCID: PMC12286868
- DOI: 10.3205/oc000253
Shield ulcer in keratoconus in the absence of atopic or vernal kerato-conjunctivitis
Abstract
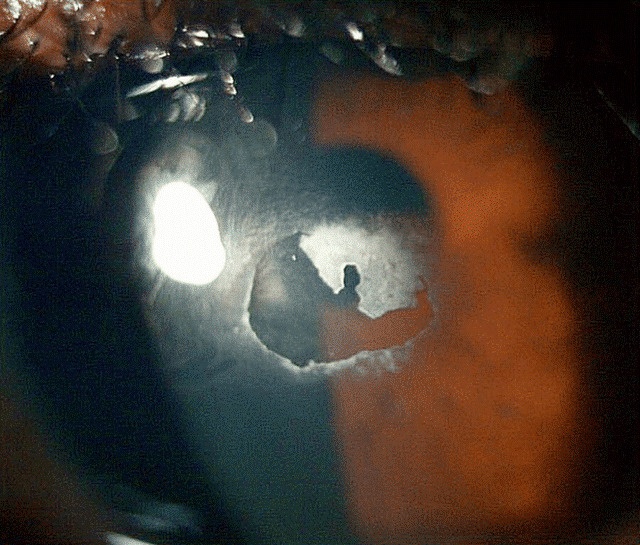
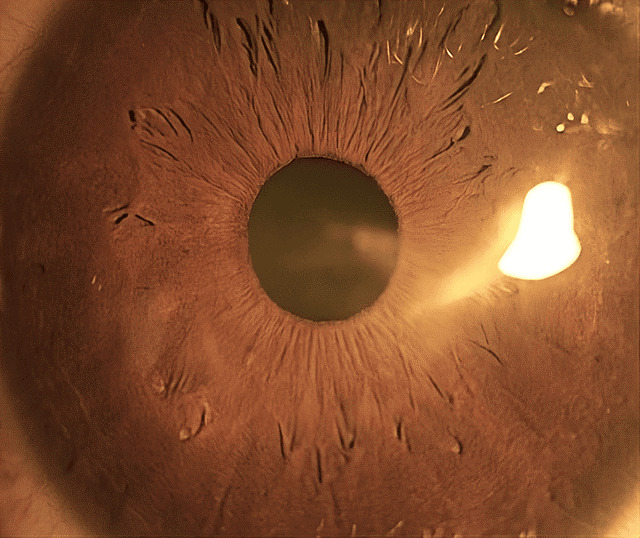
Corneal shield ulcer is a severe complication of atopic keratoconjunctivitis (AKC) and vernal keratoconjunctivitis (VKC). This condition is caused by the mechanical irritation of the corneal epithelium due to giant papillae and toxic epitheliopathy resulting from inflammatory mediators. To date, there have been no reported cases of corneal shield ulcers in the literature without AKC or VKC. However, the authors have reported a unique case of shield ulcer in a patient with keratoconus but no history of AKC or VKC. The cause is hypothesised to be due to mechanical friction between the corneal steep apex and palpebral conjunctiva. Additionally, a new technique, the use of a dry amniotic membrane, is described to manage the persistent epithelial defect in shield ulcers.
Copyright © 2025 Niestrata et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures







Similar articles
-
Topical cyclosporine for atopic keratoconjunctivitis.Cochrane Database Syst Rev. 2012 Sep 12;2012(9):CD009078. doi: 10.1002/14651858.CD009078.pub2. Cochrane Database Syst Rev. 2012. PMID: 22972132 Free PMC article.
-
Surgical Management of Corneal Sequelae of Vernal Keratoconjunctivitis.Semin Ophthalmol. 2025 Aug 30:1-10. doi: 10.1080/08820538.2025.2551061. Online ahead of print. Semin Ophthalmol. 2025. PMID: 40884264 Review.
-
Vernal Keratoconjunctivitis: A Systematic Review.Clin Rev Allergy Immunol. 2023 Aug;65(2):277-329. doi: 10.1007/s12016-023-08970-4. Epub 2023 Sep 2. Clin Rev Allergy Immunol. 2023. PMID: 37658939 Free PMC article.
-
Corneal collagen cross-linking for treating keratoconus.Cochrane Database Syst Rev. 2015 Mar 24;2015(3):CD010621. doi: 10.1002/14651858.CD010621.pub2. Cochrane Database Syst Rev. 2015. PMID: 25803325 Free PMC article.
-
Automated devices for identifying peripheral arterial disease in people with leg ulceration: an evidence synthesis and cost-effectiveness analysis.Health Technol Assess. 2024 Aug;28(37):1-158. doi: 10.3310/TWCG3912. Health Technol Assess. 2024. PMID: 39186036 Free PMC article.
References
-
- Das S. Shield ulcer: A very rare presentation. Kerala J Ophthalmol. 2017;29(3):244–246. doi: 10.4103/kjo.kjo_73_17. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
