

Navigating chronic pancreatitis pain: a pathophysiological and therapeutic overview
- PMID: 40708786
- PMCID: PMC12287759
- DOI: 10.3389/fphys.2025.1622845
Navigating chronic pancreatitis pain: a pathophysiological and therapeutic overview
Abstract
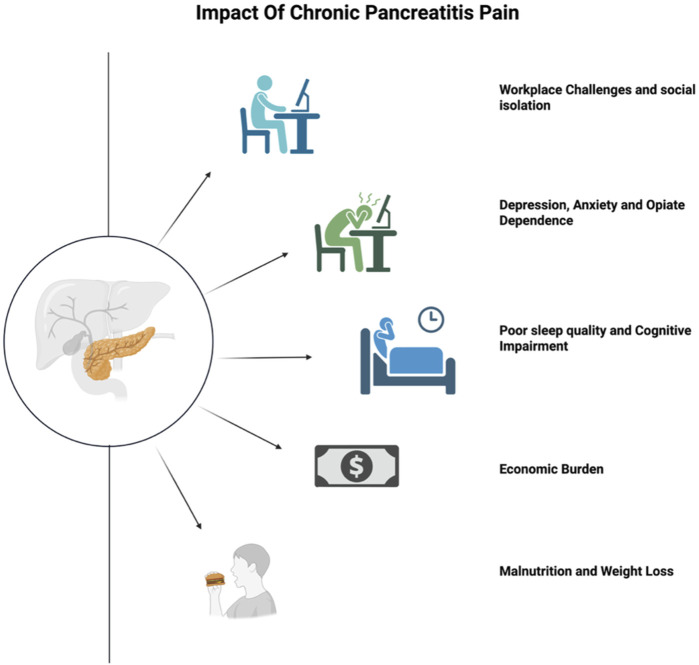
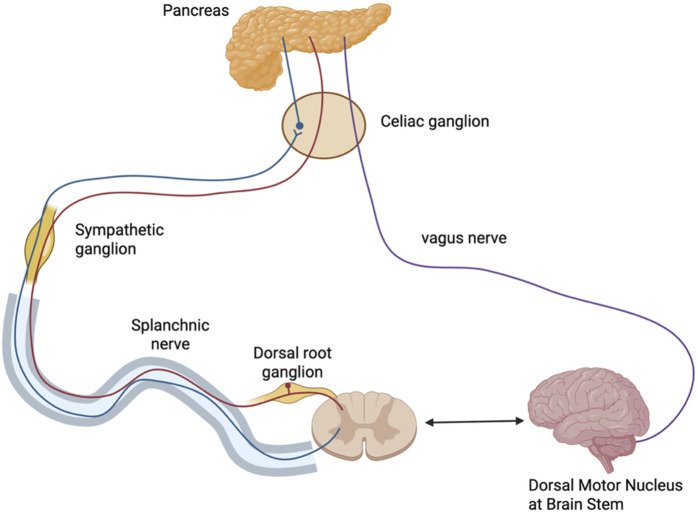
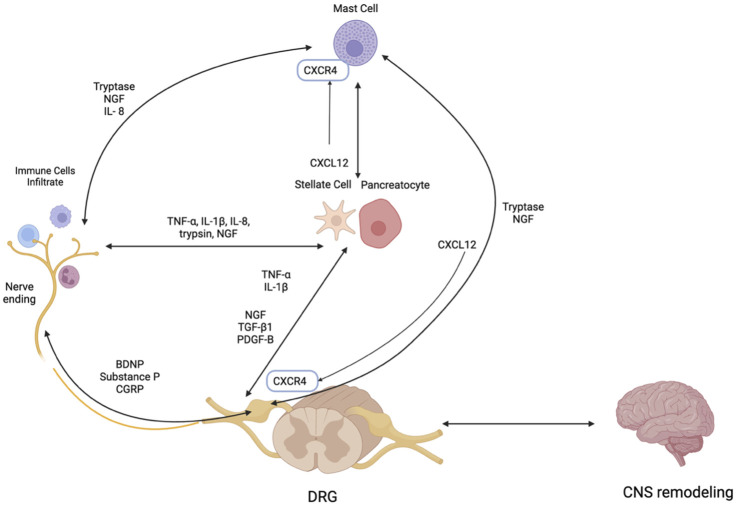
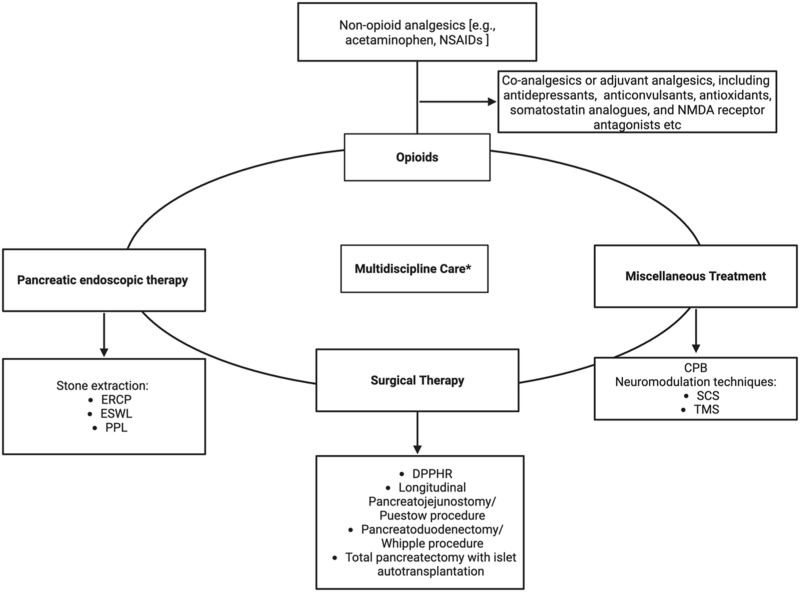
Pain management in chronic pancreatitis (CP) patients remains a major challenge, largely due to complex and refractory pain. Such pain detrimentally impacts patients by reducing quality of life, limiting daily activities, increasing psychological distress, necessitating frequent hospitalizations, and contributing to opioid dependence and socioeconomic burden. This review delineates the multifaceted nature of CP-related pain, highlighting the roles of neurogenic inflammation, maladaptive neuroplasticity, and disrupted pain modulation pathways. Current management strategies are multidisciplinary, encompassing lifestyle modification, pharmacologic therapies, endoscopic and surgical interventions, and nerve-targeted procedures (e.g., celiac plexus blocks and neurolysis). Advances in genetics, bioinformatics and biomarker research have further enhanced our understanding of CP-related pain pathogenesis, paving the way for precision medicine approaches. This review highlights current evidence and emerging innovations in the evolving landscape of CP-related pain management, emphasizing the importance of tailored and interdisciplinary care to address the intricate mechanism of CP-related pain and improve patient outcomes.
Keywords: central sensitisation; chronic pancreatitis; neurogenic inflammation; pain managemant; quality of life.
Copyright © 2025 Lin, Pandol, Apte and Jiang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous