

The association between neutrophil percentage to albumin ratio and progression-free survival and overall survival in colorectal cancer patients: a retrospective cohort study
- PMID: 40709341
- PMCID: PMC12286818
- DOI: 10.3389/fnut.2025.1589854
The association between neutrophil percentage to albumin ratio and progression-free survival and overall survival in colorectal cancer patients: a retrospective cohort study
Abstract
Background: The neutrophil percentage-to-albumin ratio (NPAR) is a promising indicator for predicting outcomes in various cancers. However, its prognostic value in colorectal cancer (CRC) is still underexplored. This study aimed to investigate the relationship between NPAR and progression-free survival (PFS) as well as overall survival (OS) in CRC patients.
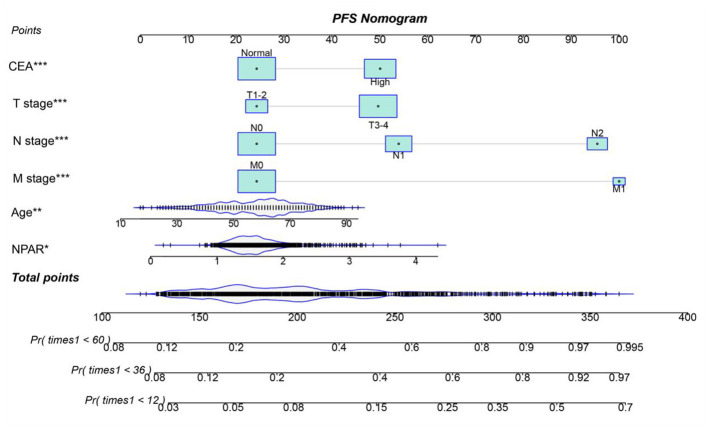
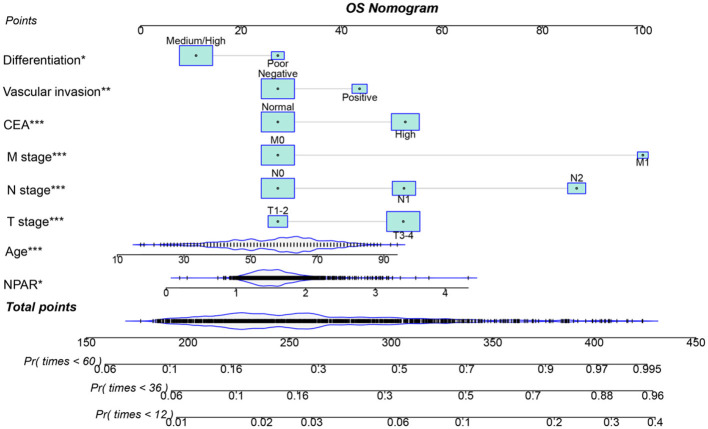
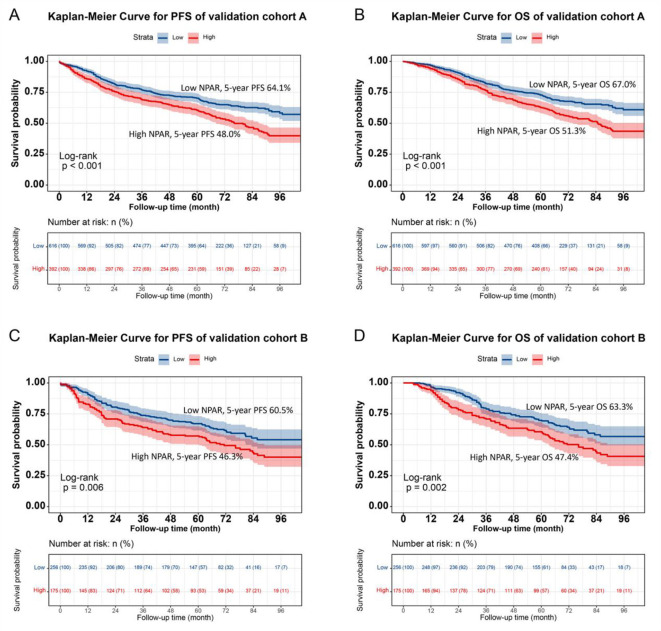
Methods: We conducted a retrospective cohort study involving 1,339 CRC patients who underwent surgical resection. The Kaplan-Meier method was utilized to plot survival curves for PFS and OS. Cox proportional hazards regression analysis assessed the relationship between NPAR and survival outcomes. The nomograms that included NPAR and other significant prognostic factors were developed to predict 1-, 3-, and 5-year survival rates.
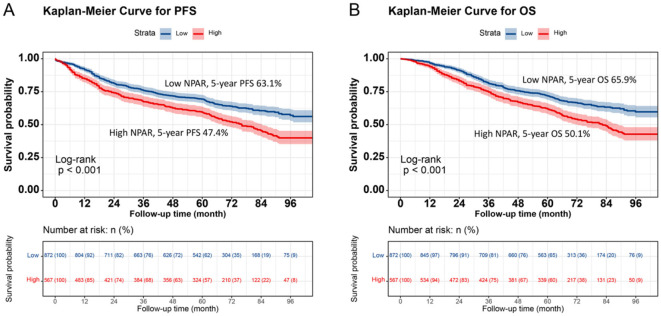
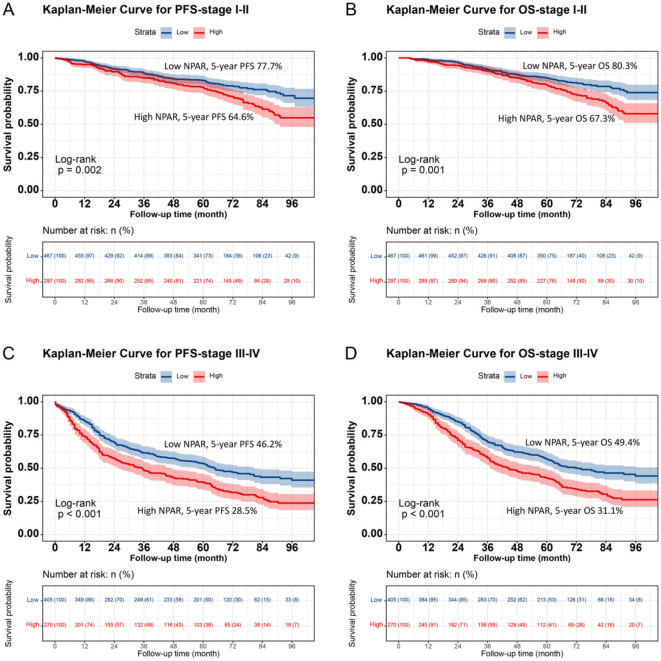
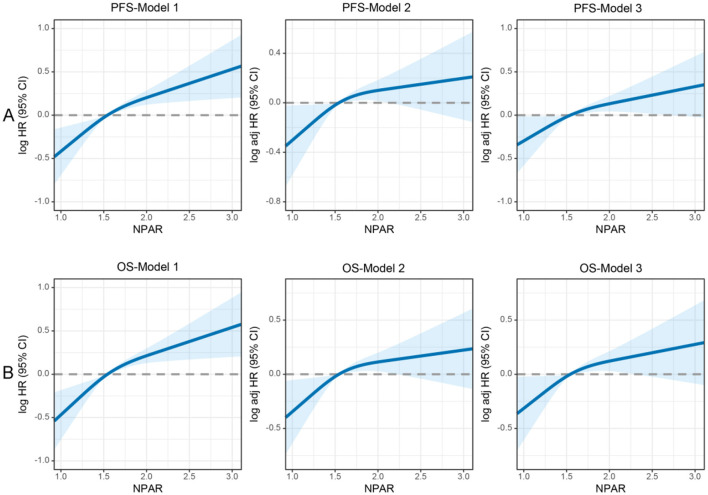
Results: Patients with high NPAR (≥1.62) experienced significantly worse PFS and OS compared to those with low NPAR (<1.62) (PFS: 47.4% vs. 63.1%, p < 0.001; OS: 50.1% vs. 65.9%, p < 0.001). Compared to other relevant markers, NPAR exhibited strong prognostic predictive efficacy. Multivariate Cox regression analysis identified high NPAR as an independent predictor of poor PFS (hazard ratio [HR] = 1.671, 95% Confidence Interval [CI]: 1.142-2.444, p = 0.008) and OS (HR = 2.697, 95% CI: 1.761-4.130, p < 0.001). The NPAR-based nomograms demonstrated high predictive accuracy and received favorable evaluations in the internal validation cohort.
Conclusion: Preoperative NPAR is a promising indicator for predicting PFS and OS in CRC patients. The NPAR-based nomogram offers a practical tool for personalized survival prediction and may assist in clinical decision-making.
Keywords: albumin; colorectal cancer; neutrophil percentage; overall survival; progression-free survival.
Copyright © 2025 Xie, Wei, Tang and Gan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources